
2 Minute Medicine Rewind February 18, 2019
With an ever-increasing aging general population, older adults have the potential to contribute to an expansion of the donor pool. Organs from older donors are typically underused, despite the present shortage of donors. Historically, liver grafts from older donors have been associated with graft loss and increased recipient mortality, thus deterring their use. In this retrospective cohort study, outcomes of graft discard, graft loss and mortality were assessed in 4127 liver grafts from older donors and 3350 liver-only recipients of older donor grafts and compared to outcomes observed in 78,990 liver grafts from younger donors and 64,907 liver-only recipients of younger donor grafts. Researchers found that liver graft discard from older donors increased from 2003-2016, while mortality rates among recipients from both older and younger donors improved after liver transplant. When comparing mortality rates for recipients of grafts in 2003-2009 with recipients in 2010-2019, investigators found greater improvements in mortality occurring for recipients of grafts from older donors (p=0.04 for interaction). Recipients who received grafts from older donors in 2010-2016 had a 41% lower mortality risk than recipients in 2003-2009 (HR 0.59, 95% CI 0.52 to 0.68, p<0.001), while mortality among recipients of grafts from younger donors improved by 31% (HR 0.69, 95% CI 0.66 to 0.71, p<0.001). In terms of graft loss, graft loss for recipients of liver grafts improved in 2010-2016 compared to 2003-2009, with greater improvements for liver grafts from older donors. From 2010-2016, recipients of liver grafts from older donors had a 40% reduced risk of graft loss (HR 0.60, 95% CI 0.53 to 0.68, p<0.001), while recipients of grafts from younger donors had a 30% improvement of graft loss (HR 0.70, 95% CI 0.68 to 0.72, p<0.001). Taken together, the results from this study suggest that despite decreased use of liver grafts from older donors, there has been an overall improvement in all-cause graft loss and mortality among recipients of liver grafts from older donors. This study is limited in that it could not assess whether the improvement in outcomes correlated with improved post-transplant care or candidate selection for older donors.
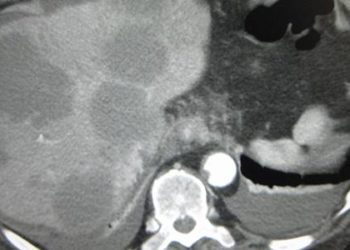
Effects of a Thermal Accelerant Gel on Microwave Ablation Zone Volumes in Lung: A Porcine Study
Image-guided thermal ablation is used as a cancer treatment modality; however, local tumor progression continues to be a problem. Thermal accelerant use has been proposed as a way of increasing microwave ablation zones in lungs in order to better achieve therapeutic oncolysis. In this preclinical study, investigators developed a thermal accelerant and randomized 9 domestic male swine to receive microwave ablations with and without thermal accelerant in order to quantify ablation zone volumes achieved. Investigators found that the use of thermal accelerant was associated with a larger average ablation zone volume of 4.3 cm3 (95% CI 3.4 to 5.5) compared to 2.1 cm3 for control ablations (95% CI 1.4 to 2.9) (p<0.001). Investigators also found that thermal accelerant use was associated with enlargement of both long- and short-axis ablation zone measurements. Percutaneous administration of thermal accelerant was associated with a larger ablation zone than endobronchial delivery (p=0.03). The standard error was lower for endobronchial delivery than for percutaneous administration (0.07 vs. 0.13, p=0.03). Overall, the results from this study provide preliminary evidence that use of a thermal accelerant may improve thermal ablation. This study is limited in that it used healthy model organisms, and long-term adverse effects were not studied.
Left ventricular mechanical dispersion predicts arrhythmic risk in mitral valve prolapse
Patients with a mitral valve prolapse (MVP) with either focal or diffuse myocardial fibrosis have been found to be at risk of cardiac arrest or sudden death, however, current diagnostic methods continue to be limited. Speckle-tracking echocardiography (STE) derived mechanical dispersion is a parameter of heterogeneous ventricular contraction, and has been proposed as a predictor of arrhythmic complications in patients with MVP. In this prospective cohort study, investigators used STE to calculate global longitudinal strain (GLS) and mechanical dispersion for 32 individuals with arrhythmic MVP (A-MVP), 27 individuals with non-arrhythmic MVP (NA-MVP) and 39 healthy controls in order to examine the association between STE results and ventricular arrhythmia. Investigators found that there were no relevant differences in baseline clinical parameters for individuals with A-MVP versus those with NA-MVP, with the exception of antiarrhythmic medication use (p=0.009). There were also no differences between the A-MVP and NA-MVP groups in terms of standard echocardiographic parameters apart from a high number of bileaflet MVPs in the A-MVP group (p=0.031). In terms of STE results, GLS was similar between the two groups (p=0.37), but mechanical dispersion was higher in the A-MVP group (mean 59 ms) than in the NA-MVP group (mean 43 ms) (p<0.001). A multivariate model including mechanical dispersion, bileaflet involvement, and MR vena contracta width showed that the mechanical dispersion was the only predictor of arrhythmic risk (OR 1.1, 95% CI 1.02 to 1.11, p=0.006). In terms of reproducibility, the correlation coefficient for mechanical dispersion was 0.80 (95% CI 0.78 to 0.87). The results from this study indicate that STE-derived mechanical dispersion is associated with arrhythmic complications, and may be used in identifying patients with higher risk.
Association between Periprocedural Neutropenia and Early Infection-related Chest Port Removal
Implantable subcutaneous chest ports are used in maintaining long-term central venous access. The use of these ports is common in a number of clinical settings, including but not limited to the receipt of chemotherapeutic agents, long-term antibiotics and immunosuppressants. There is concern, however, that neutropenia puts individuals at higher risk of subcutaneous chest port infection and early removal. In this retrospective cohort study, investigators analyzed data on 2580 patients with implantable subcutaneous chest ports in order to examine whether neutropenia status was associated with port infection. Investigators found that patients with neutropenia had a higher rate of infection-related port removal than those who were not neutropenic (3.8% vs. 0.91%, p=0.003). The neutropenic group had a higher rate of infection-related complication (4.4% vs. 1.0%, p=0.004) as well as a slightly higher incidence of death related to port infection, though this was not statistically significant (p=0.22). Taken together, the results from this study indicate that neutropenia at the time of port placement is correlated with a higher rate of infection-related complications and port removal. As such, patients with neutropenia requiring prolonged central venous access may benefit from the placement of alternative tunneled or non-tunneled central venous access until neutropenia resolves.
Association of Systemic Antibiotic Treatment of Acne With Skin Microbiota Characteristics
Systemic antibiotics are commonly used in the treatment of acne. However, the impact of their use on the complete bacterial microbiome of skin has not been well studied. In this small cohort study, investigators assessed skin samples from 4 women who were prescribed minocycline across 12 weeks in order to examine the effect of minocycline on the composition, diversity and resilience of skin microbiota associated with systemic antibiotic perturbation in individuals with acne. Investigators found that the mean relative abundance of Cutibacterium acnes decreased for all patients from baseline to week 4 of minocycline treatment (p=0.04). At 8 weeks post-discontinuation of minocycline treatment, the relative abundance of C. acnes had reverted to a level that was not statistically significant from baseline (p=0.06). Investigators found 12 genera of bacteria from skin samples showed statistically significant changes over time and had relative abundance greater than 0.1% in all samples. Five genera showed decreases in relative abundance from baseline to week 4 of treatment: Cutibacterium (p=0.04), Corynebacterium (p=0.005), Prevotella (p=0.008), Lactobacillus (p=0.02), and Porphyromonas (p=0.01). Out of these 5 genera, only Porphyromonas had relative abundances similar to baseline at week 8 after discontinuation of minocycline. There were also 7 genera that demonstrated greater relative abundance from baseline to week 4 of minocycline: Streptococcus (p=0.04), Chryseobacterium (p=0.01), Finegoldia (p=0.03), Pseudomonas (p<0.001), Erwinia (p<0.001), Actinobacillus (p=0.04), and Micrococcus (p=0.03). Streptococcus, Chryseobacterium, Finegoldia species did not have relative levels return to baseline after discontinuation of minocycline. Overall, the results of this study indicate that systemic antibiotic treatment for acne is associated with changes in the composition and diversity of skin microbiota, and variable rates of recovery across individuals. Reductions in the relative abundance of C. acnes along with the concurrent growth and suppression of certain bacterial populations has important clinical implications and may help clinicians in decreasing the likelihood of comorbidities related to microbial dysbiosis.
Image: PD
©2019 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.





{kind=link}