
2 Minute Medicine Rewind May 1, 2017
The leading cause of maternal death worldwide is post-partum hemorrhage. Tranexamic acid reduces blood loss by inhibiting plasmin in the breakdown of fibrinogen and fibrin, and has been shown to decrease bleeding in studies on surgical and trauma patients. In this randomized controlled trial, 20,060 women with post-partum hemorrhage after a vaginal birth or caesarean section were randomized to receive either 1 g intravenous tranexamic acid or matching placebo to assess the effects of early administration of tranexamic acid on death and hysterectomy in women with post-partum hemorrhage. Researchers found that the risk of death due to bleeding was significantly reduced in patients that received tranexamic acid (RR 0.78, 95% CI 0.62 to 0.98, p=0.03). Deaths due to pulmonary embolism, organ failure, sepsis, eclampsia and other causes did not significantly differ between groups. In addition, when stratified according to the timing of administration of tranexamic acid, researchers noted that there was a reduced risk of death due to bleeding if administered within 3 hours of birth (RR 0.69, 95% CI 0.52 to 0.91, p=0.008), however, there was no apparent reduction in risk if administered after 3 hours (RR 1.07, 95% CI 0.76 to 1.51, p=0.70). Researchers also found that the risk of hysterectomy was not reduced with tranexamic acid (RR 1.02, 95% CI 0.88 to 1.07, p=0.84), nor was the risk of hysterectomy to control bleeding reduced (RR 0.95, 95% CI 0.81 to 1.12, p=0.57). Furthermore, there was a significant reduction in laparotomy performed to control bleeding in the intervention group (RR 0.64, 95% CI 0.49 to 0.85, p=0.002). This study therefore shows that the administration of tranexamic acid in women with post-partum hemorrhage reduces the risk of death due to bleeding. When being used in the treatment of postpartum hemorrhage, it should be administered promptly, within 3 hours of birth, for maximal effect.
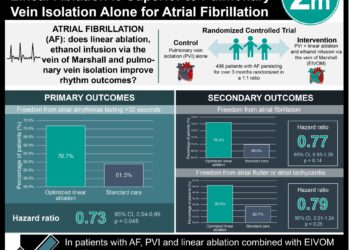
Uninterrupted dabigatran versus warfarin for ablation in atrial fibrillation
Catheter ablation can be used in the management of symptomatic atrial fibrillation, with its use dependent on previous antiarrhythmic treatment and type of atrial fibrillation. For this procedure, systemic anticoagulation before, during, and after ablation is used in reducing the risk of periprocedural adverse events, specifically stroke, transient ischemic attack (TIA) and cardiac tamponade. Uninterrupted vitamin K antagonism during the time of ablation is associated with a reduced risk of bleeding and stroke than stopping vitamin K antagonism and bridging with low molecular weight heparin. However, dabigatran has efficacy and safety outcomes that are similar, if not superior, to those of warfarin for stroke prevention in patients with atrial fibrillation. As such, in this randomized controlled trial, 635 patients undergoing catheter ablation of paroxysmal or persistent atrial fibrillation were randomized to receive dabigatran 150 mg twice daily, or warfarin (target INR 2.0-.3.0) to compare the safety and efficacy of these periprocedural anticoagulation regimens. Researchers found that the percentage of patients with major bleeding events was significantly reduced in the dabigatran group at 1.6% compared to the warfarin group at 6.9% (HR 0.22, 95% CI 0.08 to 0.59). After 8 weeks of follow-up, there were no events of stroke, systemic embolism or TIA in the dabigatran group, and only 1 event, a TIA, in the warfarin group. This study therefore shows that, in patients undergoing ablation for atrial fibrillation, anticoagulation with uninterrupted dabigatran is associated with fewer bleeding complications compared to uninterrupted warfarin.
Suicide prevention in an emergency department population: The ED-SAFE study
Suicide is a leading cause of death in the United States. The emergency department (ED) represents an important location for suicide prevention activities, as many patients at risk for suicidal behaviour seek care in these settings. In this prospective cohort study, 1376 adults with a recent suicide attempt or ideation participated in an ED-initiated suicide prevention intervention composed of 3 sequential phases: 1) treatment as usual (TAU) phase, 2) universal screening phase, 3) universal screening plus intervention phase. Participants were subsequently followed up to determine whether this intervention reduces subsequent suicidal behaviour. The intervention consisted of universal suicide risk screening, secondary suicide risk screening by the ED physician, discharge resources, and post-ED telephone calls focused on reducing suicide risk. Researchers found that during the TAU phase, 22.9% of participants made a suicide attempt, compared to 21.5% of patients in the screening phase, and 18.3% during the intervention phase. In other words, there was no appreciable difference in risk reduction between the TAU and screening phases, however, participants in the intervention phase did demonstrate some small, but meaningful reductions in suicide risk (RR 0.72, 95% CI 0.52 to 1.00, p=0.05), with a number needed to treat (NNT) of 22. This study therefore shows that, among at-risk patients in the ED, a combination of brief interventions delivered during and post-visit decreases post-ED suicidal behaviour.
Latent cytomegalovirus (CMV) infection is present in over 50% of adults. Patients primarily infected with CMV are typically asymptomatic, as the immune system acts to suppress the virus. However, if the immune response is inadequate, reactivation occurs. This is often the case in immunocompromised patients, where CMV becomes detectable in bodily fluids, placing patients at risk of a wide range of clinical problems. Due to impaired host defense mechanisms, particularly in those with a systemic inflammatory response, patients with critical illness are also at an increased risk of CMV reactivation. Several antiviral agents, including valganciclovir hydrochloride and valacyclovir hydrochloride, are used prophylactically in organ transplant recipients. However, there is no current data evaluating the use of these antiviral agents in non-immunosuppressed patients in the ICU. As such, in this randomized controlled trial, 124 CMV-seropositive patients undergoing mechanical ventilation in the intensive care unit (ICU) were randomized to receive anti-CMV prophylaxis with valacyclovir hydrochloride, low-dose valganciclovir hydrochloride or usual care for up to 28 days to assess the efficacy, safety and feasibility of antiviral prophylaxis for suppressing CMV reactivation in critically ill patients receiving care in the ICU. Researchers found that CMV reactivation was significantly less likely in patients that received an antiviral agent compared to placebo (HR 0.14, 95% CI 0.04 to 0.50, p=0.002). An analysis of secondary outcomes revealed that there was no significant difference with respect to in-hospital mortality when comparing the valganciclovir and control groups (RR 1.3, 95% CI 0.6 to 2.7), however, there was some increased risk for those assigned to the valacyclovir group (RR 2.2, 95% CI 1.1 to 4.3). The authors also examined the risk of experiencing a serious adverse event and found that patients administered valacyclovir (RR 1.8, 95% CI 0.8 to 4.4) or valganciclovir (RR 2.2, 95% CI 1.0 to 4.8) were not at a significantly increased risk of experiencing a serious adverse event. This study therefore shows that antiviral prophylaxis with valacyclovir or low-dose valganciclovir suppresses CMV reactivation in critically ill patients. As the administration of valacyclovir is associated with increased in-hospital mortality, however, further studies are required to determine the clinical efficacy and safety of CMV suppression.
Higher surgical morbidity for ulcerative colitis patients in the era of biologics
The use of biologic therapy in the management of ulcerative colitis (UC) has allowed patients with moderate to severe disease to achieve clinical remission where conventional therapies have failed. Based on the results of several randomized controlled trials, biologics, such as infliximab, may also reduce the short-term need for surgery. However, 30-66% of patients treated with biologics still ultimately require surgery. In this retrospective cohort study, 7070 patients that had undergone surgery for UC were studied to investigate the impact of biologic therapy on postoperative outcomes. Patients were stratified by date, as biologic therapy was introduced in 2005. Researchers found that patients undergoing surgery after 2005 had higher rates of in-hospital mortality (8.1% vs. 5.5%), major adverse events (7.4% vs. 5.3%) and procedural complications (12.3% vs. 9.9%) compared to patients that received surgery before 2005 (p<0.01). Upon adjusting for important confounders, including comorbidities, emergent or urgent surgery and sex, the authors found that patients undergoing surgery after 2005 were more likely to experience major events (OR 1.39, 95% CI 1.11 to 1.75), procedural complications (OR 1.40, 95% CI 1.19 to 1.66), transfusion (OR 1.15, 95% CI 1.02 to 1.31) and non-routine discharge (OR 3.10, 95% CI 2.73 to 3.52). In comparing patients who received elective surgery only, patients who had surgery after 2005 had a higher adjusted risk of 90-day readmission (OR 1.33, 95% CI 1.14 to 1.55), major events (OR 1.67, 95% CI 1.18 to 2.35) and procedural complications (OR 1.58, 95% CI 1.29 to 1.95). This study therefore shows that, in keeping with the introduction of biologic agents in 2005, patients with UC that have received biologic therapy may be at an increased risk of postoperative morbidity.
Image: PD
©2017 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.





{kind=link}