
2 Minute Medicine Rewind November 30, 2015
Home Use of an Artificial Beta Cell in Type 1 Diabetes
While intensive insulin therapy is the standard of care for type 1 diabetes, it is limited by the need for active management and the risk of hypoglycemia. The concept of sensor-responsive insulin delivery was developed to combat this challenge and the artificial beta cell, or closed-loop insulin-delivery system, expands on this concept by algorithmically and continuously increases or decreases the subcutaneous delivery of insulin based on real-time glucose levels. However, the safety and efficacy of prolonged use of an artificial beta cell in the home setting have not been established. This study was a two center, crossover, randomized control study conducted under free-living home conditions that compared closed-loop insulin delivery versus standard sensor-augmented pump. 58 patients were assigned to 12 weeks of closed-loop therapy and then to 12 weeks of standard therapy or vice versa. The primary end point was the proportion of time that the glucose level was between 70 mg and 180 mg per deciliter for adults and between 70 mg and 145 mg per deciliter for children and adolescents. Results showed that the rate of primary outcome was higher with the closed-loop system versus control in adults (Difference 11%; 95% CI 8.1 to 13.8; p<0.001). Furthermore, the mean glucose level was lower during the closed-loop phase (Difference −11 m/dL, 95% CI: −17 to −6, p<0.001) as was the mean glycated hemoglobin level (Difference −0.3%; 95% CI −0.5 to −0.1; p=0.002). Among children, the rate of primary outcome was also higher (Difference 24.7%; 95% CI 20.6 to 28.7; p <0.001). Overall, this was an excellent study only limited by the number of devices each participant had to use. In conclusion, use of a closed-loop system at home over a period of 12 weeks without close supervision is feasible in adults, children, and adolescents with type 1 diabetes. Furthermore, preliminary results show better glycemic control and reduced burden of hypoglycemia with the closed-loop system.
Despite a lack of sound evidence, oral fluoropyrimidines are often used as the first-line treatment of metastatic breast cancer to avoid severe adverse side effects associated intravenous chemotherapy. The SELECT BC trial, was a phase 3 non-inferiority, randomized trial that compared oral fluoropyrimidine S-1 (containing tegafur, gimeracil, and oteracil) versus taxane as first line chemotherapy for HER2-negative metastatic breast cancer. 618 patients across 154 Japanese hospitals were randomly assigned in a 1:1 fashion to taxane (n=309, docetaxel 60–75 mg/m2 at intervals of 3–4 weeks; paclitaxel 80–100 mg/m2 weekly for 3 of 4 weeks; or paclitaxel 175 mg/m2 at intervals of 3–4 weeks) or to S-1 (n=309, 40–60 mg twice daily for 28 consecutive days, followed by a 14-day break). The primary endpoint was overall survival with a non-inferiority margin hazard ratio of 1.333. Results showed a median overall survival of 35.0 months (95% CI 31.1 to 39.0) in the S-1 group and 37.2 months (95% CI 33.0 to 40.1) in the taxane group (Hazard ratio 1.05; 95% CI 0.86 to 1.27; p=0.015 for non-inferiority). The most common side effects were neutropenia (7% vs 3%), fatigue (3% vs 4%) and edema (<1% vs 4%) in the S-1 vs taxane groups respectively. In conclusion, this study showed that S-1 is non-inferior to taxane with respect to overall survival as a first-line treatment for metastatic breast cancer in HER2-negative patients.
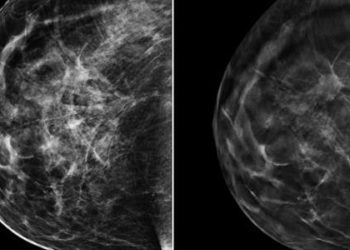
Panretinal Photocoagulation vs Intravitreous Ranibizumab for Proliferative Diabetic Retinopathy
Panretinal photocoagulation (PRP) is the standard of care for proliferative diabetic retinopathy (PDR). However, PRP can cause permanent peripheral visual field loss, decreased night vision and can worsen diabetic macular edema. Intravenous anti-VEGF agents are thought to be potential agents for treating PDR. This study was a multicenter, randomized clinical trial across 55 US centers, involving 394 patients that evaluated ranibizumab compared to PRP for visual acuity outcomes in patients with PDR. The primary outcome was mean visual acuity change at 2 years. Results indicated that mean visual acuity letter improvement at 2 years was +2.8 in the ranibizumab group versus +0.2 in the PRP group (Adjusted Difference +2.2; 95% CI -0.5 to +5.0; p<0.001 for non-inferiority). In the PRP group vs the ranibizumab group, mean peripheral visual field sensitivity loss was worse (−23 dB vs −422 dB; Difference 372 dB; 95% CI 213 to 531 dB; p < .001) and DME macular edema development was more frequent (28% vs 9%, Difference 19%; 95% CI 10% to 28%; p < 0.001). However, eyes without active or regressed neovascularization was not significantly different between the ranibizumab vs PRP groups (Difference 3%; 95% CI −7% to 12%; p = 0.58). The main limitation of this study was the lack of blinding as the nature of the treatments precluded masking participants and clinicians. Secondly, there was less than expected 2-year follow-up. In conclusion, this study showed that in patients with PDR, use of ranibizumab was noninferior to PRP in regards to visual acuity at the 2 year mark.
Nucleoside reverse transcriptase inhibitors (NRTIs) are often used in anti-retroviral regimens for patient with HIV. However, there is insufficient data regarding their necessity in treatment-experienced patients and those with viral resistance. This study was a multicenter, randomized controlled trial involving 360 patients across outpatient HIV clinics that compared success between patients who omit versus receive NRTIs, in addition to an optimized antiretroviral regimen of 3 or more agents. The primary endpoint was regimen failure, using a non-inferiority margin of 15%, through 48 weeks. The primary safety endpoint was time to initial episode of severe symptoms or laboratory abnormalities, such as threshold HIV RNA levels. The 360 patients were randomized to receive versus not receive NRTIs as a part of their HAART regimen and were followed through 48 weeks, with 93% successful follow-up. Results showed a probability of regimen failure of 29.8% vs 25.9% in the omit-NRTIs vs add-NRTIs groups respectively (Difference 3.2%; 95% CI −6.1% to 12.5%). Furthermore, no significant differences were found between the two groups in regards to safety endpoints. There were also no differences between the proportions of patients with HIV RNA levels of less than 50 copies/mL. Although an excellent study, the lack of blinding was the major limitation of this trial. In conclusion, this study showed than in treatment-experienced patients with HIV, NRTIs can be safely omitted without a compromise in virologic efficacy.
Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes
Although Type 2 diabetes is a major risk factor for cardiovascular disease, there is unconvincing evidence that lowering blood glucose reduces rates of cardiovascular mortality. This study was a randomized, double-blind, placebo-controlled trial to assess the effect of once-daily empagliflozin, an inhibitor or sodium-glucose cotransporter 2, in reducing cardiovascular events in high risk adults with type 2 diabetes. 7020 patients were randomly assigned to receive 10 mg or 25 mg of empagliflozin or placebo once daily. The primary outcome was a death from cardiovascular causes, nonfatal myocardial infarction (excluding silent myocardial infarction), or nonfatal stroke. Results showed that the primary outcome occurred in 490 of 4687 patients (10.5%) in the pooled empagliflozin group and in 282 of 2333 patients (12.1%) in the placebo group, (Hazard Ratio 0.86; 95.02% CI 0.74 to 0.99; p=0.04 for superiority). In the empagliflozin group, there were significantly lower rates of death from cardiovascular causes (3.7%, vs 5.9% in the placebo group; Relative risk reduction 38%). No significant differences were found in regards to myocardial infarction or stroke. The main limitation of this study was failure of many patients to reach glycemic targets with adjusted mean glycated hemoglobin level at week 206 of 7.81% in the pooled empagliflozin group and 8.16% in the placebo group. In conclusion, patients with type 2 diabetes at high risk for cardiovascular events had significantly lower rates of primary composite cardiovascular outcomes and death in the empagliflozin group versus placebo.
Image: PD
©2015 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.





{kind=link}