
New vaccine shown to prevent a significant number of malaria cases in phase 3 trial
1. In this phase 3, randomized controlled trial, the candidate vaccine RTS,S/AS01 with or without a booster dose prevented a substantial number of clinical malaria cases in infants and children over a 3-4 year period, with increased vaccine efficacy and prolonged effect with the addition of a booster dose.
2. Severe adverse events were balanced between groups with the exception of meningitis, which occurred more frequently in RTS,S/AS01 recipients than with control vaccines.
Evidence Rating Level: 1 (Excellent)
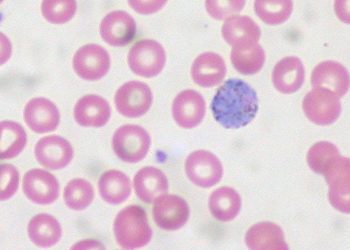
Study Rundown: Malaria is now almost completely eradicated in the industrialized world, yet unfortunately still causes significant morbidity and mortality in developing countries where health care and sanitation infrastructures are often inadequate. The disease burden is heavy in children of 6 months to 5 years of age. Classically, malaria primarily involves the liver (exoerythrocytic phase) and red blood cells (erythrocytic phase). Cerebral involvement, commonly related to P falciparum, is especially concerning in the pediatric population due to potential long-term sequelae. Published today in the Lancet are the final results of a phase 3, randomized controlled trial for the candidate vaccine RTS,S/AS01 against malaria.
Over a period of 3-4 years, the candidate vaccine was found to prevent a substantial number of clinical malaria cases in young infants and children, with vaccine efficacy of approximately 20-40% (see In-Depth for specific break-downs), including increased efficacy and prolonged protective effect in those that received a booster dose at month 20. The vaccination appeared ineffective against severe malaria in children without a booster dose and in young infants with or without a booster dose. The frequency of severe adverse events were balanced between groups; however, there were 22 cases of meningitis in children: 21 in RTS,S/AS01 recipients and 1 in a control vaccine recipient. The study was a well-designed randomized controlled trial and was adequately powered to assess vaccine efficacy. Future studies are needed to assess ways to further improve vaccine efficacy.
The study was funded by GlaxoSmithKline Biologicals SA and the PATH Malaria Vaccine Initiative.
Click to read the study in the Lancet
Relevant Reading: First results of phase 3 trial of RTA,S/AS01 malaria vaccine in African children
In-Depth [randomized controlled trial]: This study reports the final results of a phase 3, individual randomized controlled trial of the candidate malaria vaccine RTS,S/AS01, conducted between March 2009 and January 2014. The intention-to-treat analyses included 8,922 children (aged 5-17 months) and 6,537 young infants (aged 6-12 weeks) at 11 centers in 7 countries in sub-Saharan Africa. Participants were randomized 1:1:1 to 3 groups – R3R (RTS,S/AS01 at months 0, 1, and 2; booster dose at month 20), R3C (RTS,S/AS01 at months 0, 1, and 2, and control vaccine Menjugate [meningococcal serogroup C conjugate vaccine] at month 20), and C3C (comparable control vaccines at months 0, 1, 2, and 20 [rabies vaccine Verorab for children and Menjugate for young infants]). Co-primary endpoints on vaccine efficacy (VE) were published previously. This report presented data for the VE of the booster shot on the occurrence of clinical and severe malaria. Children were followed for a median of 48 months and young infants for a median of 38 months after the first dose.
In the children subgroup:
In the modified intention-to-treat population, VE against clinical malaria was 36.3% (95% confidence interval [CI] 31.8–40.5) in the R3R group and 28.3% (23.3–32.9) in the R3C group. Efficacy decreased over time and was no longer measurable in the R3C group from month 33 to the study end (VE 2.9%, 95% CI -6.4–11.4). Administration of a booster dose appeared to prolong the protective effects with VE of 12.3% (3.6-20.1) in the R3R group by study end. VE against severe malaria was 32.2% (13.7-46.9) in the R3R group and 1.1% (-23.0–20.5) in the R3C group. It was estimated that 1774 (1387–2186) cases of clinical malaria per 1000 children in the R3R group and 1363 (995–1797) cases per 1000 children in the R3C group were avoided.
In the young infant subgroup:
In the modified intention-to-treat population, VE against clinical malaria was 25.9% (19.9–31.5) in the R3R group and 18.3% (11.7–24.4) in the R3C group. Efficacy decreased over time and was no longer detectable in the R3C group by study end (VE 4.4%, -6.7–14.3). Administration of a booster dose appeared to prolong the protective effects with VE of 10.5% (0.2-19.7) in the R3R group by study end. VE against severe malaria was 17.3% (9.4-37.5) in the R3R group and 10.3% (-17.9–31.8) in the R3C group. It was estimated that 983 (592–1337) cases of clinical malaria per 1,000 young infants in the R3R group and 558 (158–926) cases per 1000 young infants in the R3C group were avoided.
In safety analyses, the incidence of generalized convulsive seizures in children within 7 days of a booster dose was 2.5 per 1000 doses in the R3R group, 1.2 per 1000 doses in the R3C group, and 0.4 per 1000 doses in the C3C group. The corresponding data for young infants were 2.2, 0.0, and 0.5, respectively. Meningitis was reported as severe adverse events in 22 children: 11 for R3R, 10 for r3C, and 1 for C3C. There was no imbalance of meningitis in the young infant group.
Image: PD
©2015 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.





{kind=link}