No products in the cart.

Fleischner Society Guidelines, 2017 Update: Consolidated follow-up recommendations for incidental solid and subsolid pulmonary nodules [Classics Series]
The following study summary is an excerpt from the book 2 Minute Medicine’s The Classics in Radiology: Summaries of Clinically Relevant & Recent Landmark Studies, 1e (The Classics Series).
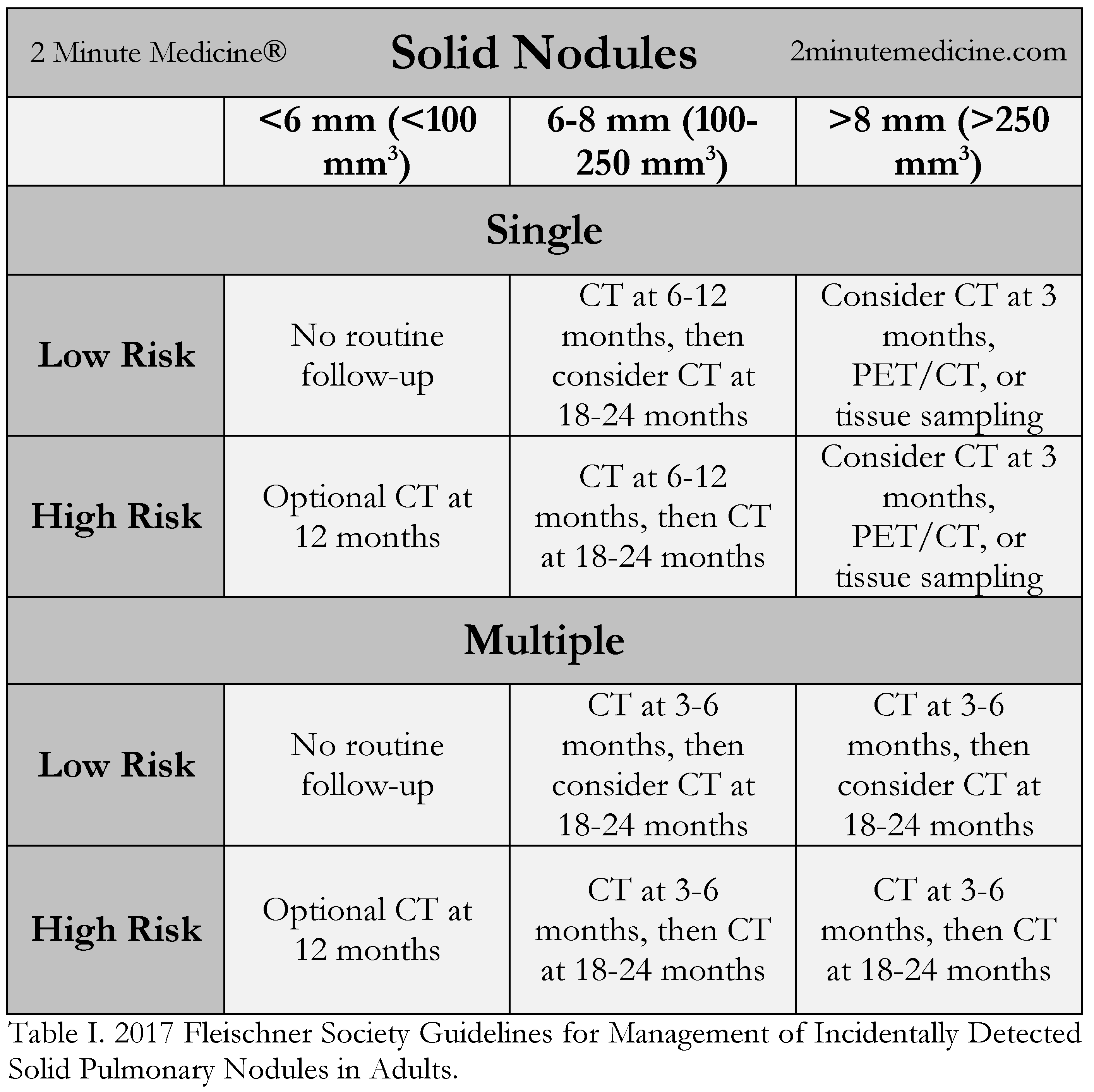
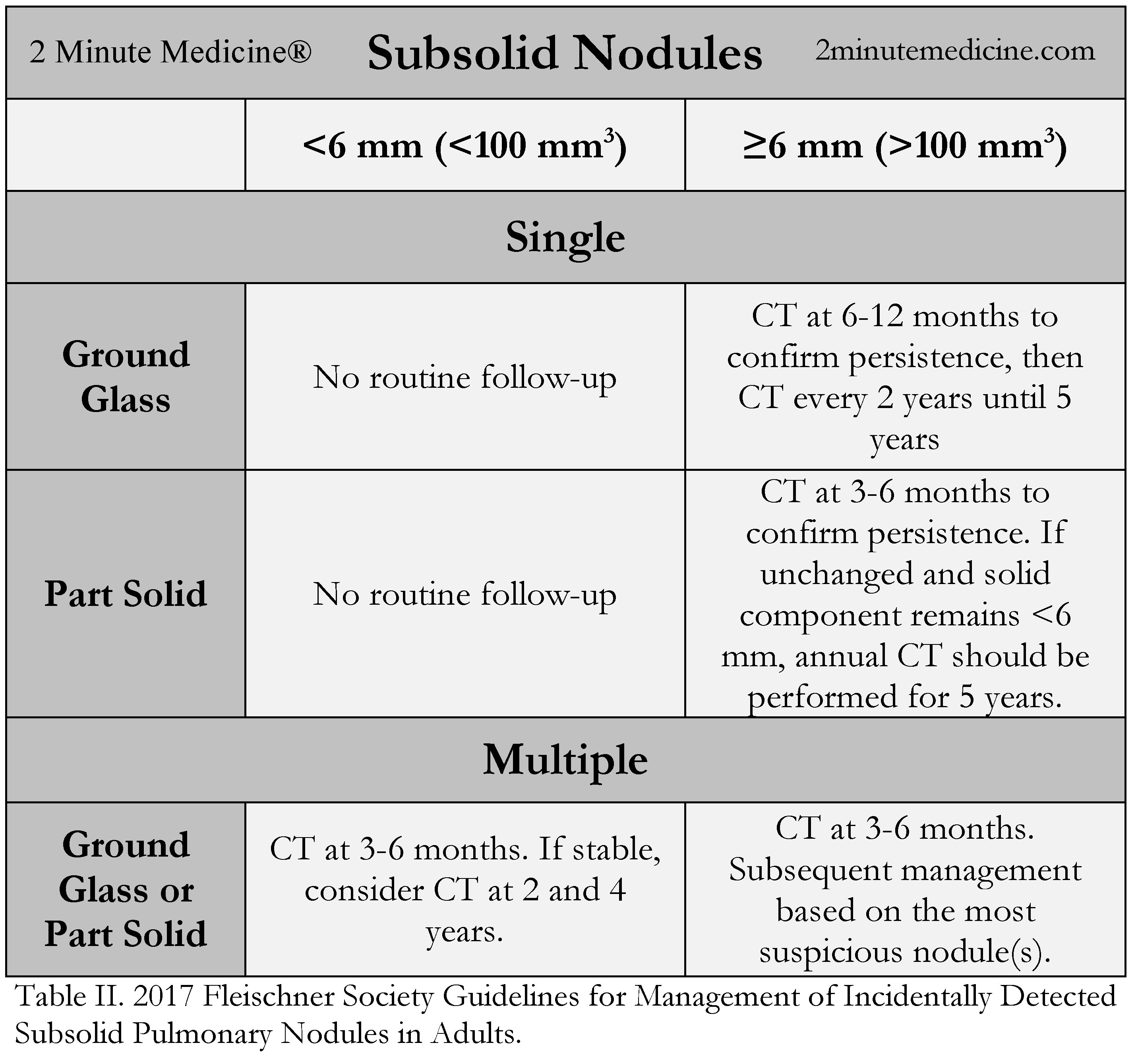
1. The revised Fleischner Society Guidelines (Tables I and II) have reduced the number of unnecessary follow-up examinations required for solid and subsolid nodules and adopted follow-up ranges to provide greater discretion in clinical decision-making.
2. In patients with a low clinical risk for lung cancer, incidentally discovered nodules (solitary or multiple) smaller than 6 mm (< 100 mm3) on computed tomography (CT) do not require additional follow-up; in patients at high risk, an optional CT at 12 months is recommended.
5. No routine follow-up is recommended for ground-glass nodules (GGNs) and part-solid nodules smaller than 6 mm (< 100 mm3); follow-up until 5 years is recommended for those larger than 6 mm (> 100 mm3).
4. Risk factors for malignancy include nodule size, tobacco and other known carcinogens, family history, upper lobe location, emphysema, and pulmonary fibrosis.
Original Date of Publication: March 2017
Study Rundown: The increased use of CT in clinical practice has increased the number of incidentally discovered pulmonary nodules. These nodules can pose diagnostic dilemmas for the radiologist given the wide differential of benign and malignant etiologies. This may result in unnecessary scans and excessive ionizing radiation exposure to patients for nodules with little malignant potential. The original Fleischner Society Guidelines, published in 2005, were evidence-based recommendations regarding follow-up periods for incidentally found solid lung nodules based on size, baseline clinical risk, and nodule morphology. Complementary guidelines for subsolid nodules were issued in 2013 after it was recognized that these unique nodules carried a distinct prognosis. The updated guidelines, published in 2017, considers critical new evidence from recent, international, multi-center lung cancer screening trials in its revisions (Table 1). The new evidence is reflected in the following major changes from the original guidelines:
- For solid nodules, the minimum size threshold that requires routine follow-up has been increased from 4 mm to 6 mm for both high and low-risk patients.
- Solitary or multiple solid nodules smaller than 6 mm (< 100 mm3) do not require additional follow-up in low risk patients; in high risk patients, an optional CT at 12 months is recommended. Stable solid pulmonary nodules between 6 mm to 8 mm require only one follow-up examination.
- For solitary part-solid and GGN, a longer initial follow-up period is recommended, and the total duration of follow-up has been increased to 5 years.
- Follow-up recommendations for both solid and subsolid nodules are provided as a range of time rather than specific time intervals, in order to incorporate various potential clinical risk factors as well as patient preference in determining management.
- Volumetric thresholds have also been established corresponding to various size criteria for solid and subsolid pulmonary nodules.
Compared to the original guidelines, recent data support a less aggressive approach in the management of small solid and subsolid pulmonary nodules. The Fleischner Society constructed these guidelines based on foundational and recent literature demonstrating several key observations:
- Patients with solid nodules smaller than 6 mm have been shown to have a cancer risk of less than 1%, even in high-risk patient populations.
- Volume doubling times for malignant solid pulmonary nodules have been well established in the 100-400 day range, while malignant subsolid nodules may present with a doubling time on the order of 3-5 years.
- Several clinical and radiographical risk factors important in the assessment of low versus high risk must be considered in establishing follow-up periods:
- Size is a dominant factor in the malignant potential of nodules.
- Nodule morphology correlates with malignant likelihood and growth rate (i.e., marginal spiculation and subsolid composition).
- Lung cancer occurs more often in the upper lobes, with a preference for the right lung.
- Emphysema and pulmonary fibrosis (especially idiopathic) are independent risk factors for malignancy.
- Cigarette smoking portends a greater risk of lethal cancers, increasing in proportion to the degree of smoking.
- Nodules in cigarette smokers grow faster than in nonsmokers.
- Malignant risk of nodules increases with patient age.
Low-risk patients are defined as patients with a minimal or absent smoking history and absence of other known risk factors including a history of lung cancer in a first-degree relative, exposure to carcinogenic material (i.e., asbestos, radon, and uranium), upper lobe location, emphysema, or pulmonary fibrosis. Conversely, high-risk patients are defined as patients with a history of smoking or the aforementioned known risk factors.
The guidelines do not apply to patients with known or suspected cancers outside of the lungs, patients younger than 35 years of age, immunocompromised patients, or patients undergoing lung cancer screening. For lung cancer screening, adherence to Lung-RADS (summarized “II. Screening Literature”), a classification system specifically designed for the subset of patients meeting screening eligibility criteria, is recommended.
Click to read the study in Radiology
MacMahon H, Naidich DP, Goo JM, Lee KS, Leung AN, Mayo JR, Mehta AC, Ohno Y, Powell CA, Prokop M, Rubin GD. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017. Radiology. 2017 Feb 23:161659.
Additional Review:
Pinsky PF, Gierada DS, Black W, Munden R, Nath H, Aberle D, et al. Performance of Lung-RADS in the National Lung Screening Trial A Retrospective Assessment Performance of Lung-RADS in the NLST. Ann Intern Med. 2015 Apr 7;162(7):485–91.
©2018 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
![The ABCD2 score: Risk of stroke after Transient Ischemic Attack (TIA) [Classics Series]](data:image/svg+xml;nitro-empty-id=Nzg2OjEzOTg=-1;base64,PHN2ZyB2aWV3Qm94PSIwIDAgMSAxIiB3aWR0aD0iMSIgaGVpZ2h0PSIxIiB4bWxucz0iaHR0cDovL3d3dy53My5vcmcvMjAwMC9zdmciPjwvc3ZnPg==)
![The ABCD2 score: Risk of stroke after Transient Ischemic Attack (TIA) [Classics Series]](data:image/svg+xml;nitro-empty-id=ODAwOjE0MjI=-1;base64,PHN2ZyB2aWV3Qm94PSIwIDAgMSAxIiB3aWR0aD0iMSIgaGVpZ2h0PSIxIiB4bWxucz0iaHR0cDovL3d3dy53My5vcmcvMjAwMC9zdmciPjwvc3ZnPg==)



{kind=link}