


![Tumor-specific mutant antigens are potential targets for cancer therapy [PreClinical]](https://www.2minutemedicine.com/wp-content/uploads/2014/12/mouse-e1417555547919-75x75.jpg)

{kind=link}


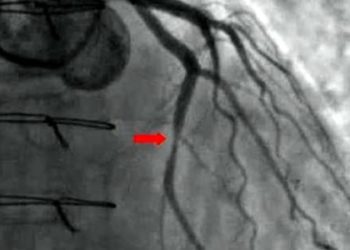
Adverse outcomes are similar for patients undergoing percutaneous coronary intervention receiving heparin or bivalirudin
1. Patients undergoing percutaneous coronary intervention (PCI) mainly via radial approach receiving either bivalirudin or heparin, in addition to P2Y12 inhibitors, following myocardial infarction experienced similar rates of death from any cause, myocardial infarction, or major bleeding.
2. Patients who had ST-segment elevation myocardial infarction (STEMI) or non-STEMI myocardial infarctions experienced similar rates of major adverse events regardless of their treatment with bivalirudin or heparin during PCI.
Evidence Rating: 1 (Excellent)
Study Rundown: Following myocardial infarction, anticoagulation and antiplatelet agents are used during PCI to improve clinical outcomes by reducing thrombotic complications. Advantages of anticoagulation and antiplatelet agents must be weighted with their adverse effects of bleeding complications. In this study, patients post myocardial infarction undergoing radial-artery PCI and receiving a potent P2Y12 inhibitor were treated with the anticoagulants heparin or bivalirudin. The primary endpoints of the study were death from any cause, myocardial infarction, and major bleeding events. This multicenter, randomized trial included patients with both STEMI and non-STEMI myocardial infarction with an urgently planned PCI. Most patients had a radial-artery PCI approach, and all were treated with P2Y12 inhibitors ticagrelor, prasugrel, or cangrelor. No significant differences in rates of primary endpoints were observed between patients treated with bivalirudin or heparin at either 30 or 180 days post-PCI. No difference in outcomes was was observed between treatment groups for patients with either STEMI or non-STEMI myocardial infarctions. The size of the study is a significant strength, while a notable weakness is many patients were allowed in the trial design to be treated with a small dose of heparin before randomization into the two treatment groups, possibly limiting the study’s ability to detect a difference in outcomes between treatment groups.
Click to read the study, published in NEJM
Relevant Reading: Bivalirudin during primary PCI in acute myocardial infarction
In-Depth [randomized controlled trial]: This multicenter, randomized controlled trial was conducted between 2014 and 2016 in Sweden. Patients post myocardial infarction (n = 3005 with STEMI; n = 3001 with non-STEMI) were randomized in a 1:1 manner to receive either bivalirudin (n = 3004) or heparin (n = 3002) anticoagulant treatment. Eligible patients had urgent PCIs planned for myocardial infarction and were treated with the potent P2Y12 inhibitors ticagrelor, prasugrel, or cangrelor. Patients received recommended doses of bivalirudin or heparin, and were allowed a small dose of heparin (<3000 U) prior to PCI in accordance with local practices. Primary end points of the study were death from any cause, myocardial infarction, or major bleeding, and outcomes were assessed at 30 and 180 days after PCI. At both 30 and 180 days after PCI, no statistical differences were measured between the treatment groups for rates of death from any cause (1.9% and 2.9% vs 1.7% and 2.8% for bivalirudin and heparin groups at 30 and 180 days, respectively), myocardial infarction (0.9% and 2.0% vs 1.1% and 2.4%), major bleeding events (5.1% and 8.6% vs 5.6% and 8.6%), or stent thrombosis (p > 0.05 for all comparisons). No differences in primary outcomes were observed between treatment groups for patients with STEMI (HR 0.96, 95%CI 0.78-1.18) or non-STEMIs (HR 0.95, 95%CI 0.78-1.17). Subgroup analysis comparing primary outcomes between the two treatment groups also showed no significant differences when accounting for sex (male and female), age (>65 and <65), history of prior myocardial infarction (yes and no), or smoking status (yes and no).
Image: PD
©2017 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports
