
Apatinib plus pegylated liposomal doxorubicin as an alternative treatment option in platinum-resistant ovarian cancer
1. Apatinib plus pegylated liposomal doxorubicin led to longer overall survival and progression-free survival, and a higher objective response rate and disease control rate.
2. Adverse events of grades 3 or higher occurred more in the combination group, with decreased neutrophil counts, hypertension, and decreased white blood cell counts being the most frequent.
Evidence Rating Level: 1 (Excellent)
Study Rundown: Previous trials have shown that the addition of an anti-vascular endothelial growth factor (VEGF) monoclonal antibody to non-platinum-based chemotherapy had some anti-cancer benefits. In refractory ovarian cancer, platinum resistance (PROC) is a common mechanism and therefore chemotherapy with anti-VEGF therapy is an investigational option. This study explored the efficacy and safety of apatinib (a VEGF receptor 2 tyrosine kinase inhibitor) plus pegylated liposomal doxorubicin (PLD) on platinum-resistant ovarian cancer (PROC). Patients were randomly assigned to receive apatinib plus PLD or PLD alone. In the combination group, the median progression-free survival (PFS) and median overall survival (OS) were longer, while the objective response rate (ORR) and disease control rate (DCR) was higher. Adverse events were consistent with the published safety profiles of apatinib plus chemotherapy in ovarian cancer and other tumours. The most common treatment-emergent adverse events of any grade in both groups were decreased white blood cell and neutrophil counts. Adverse events of grades 3 or higher occurred more in the combination group, whereby decreased neutrophil counts, hypertension, and decreased white blood cell counts were the most frequent. Limitations to this study include its generalizability as it only examined Chinese patients. Also, the OS events were immature in the combination group and quality of life was not examined. The strength of this study is that it has limited bias given its design and that apatinib can be taken orally in comparison to the intravenous administration of other VEGF inhibitors. Overall, the addition of apatinib to PLD showed clinical benefit and can be an alternative treatment option for PROC.
Click to read the study in JAMA Oncology
Relevant Reading: Bevacizumab combined with chemotherapy for platinum-resistant recurrent ovarian cancer: the aurelia open-label randomized phase iii trial
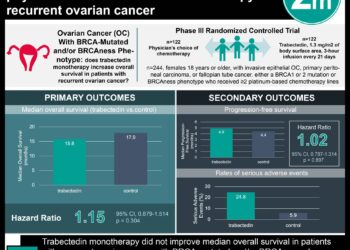
In-Depth [randomized control trial]: This multicenter randomized clinical trial in China randomly assigned 152 patients to receive either apatinib with PLD, or PLD alone; 78 in the combination group and 74 in the PLD arm. Median PFS for the combination group was 5.8 months (95% confidence interval [CI], 3.8 to 8.8) and 3.3 months (95% CI, 2.1 to 3.8) for the PLD arm (hazard ratio [HR], 0.44; 95% CI, 0.28 to 0.71; P<0.001). Median OS for the combination group was 23.0 months (95% CI, 18.9 to not reached) and 14.4 months (95% CI, 12.1 to 23.4) for the PLD arm (HR, 0.66; 95% CI, 0.40 to 1.09). ORR was achieved in 43.1% (95% CI, 30.8% to 56.0%) and 10.9% (95% CI, 4.5% to 21.2%) of patients in the combination group and single-arm, respectively. The DCR was 81.5% (95% CI, 70.0% to 90.1%) and 53.1% (95% CI, 40.2% to 65.7%) for the combination group and single-arm, respectively (rate difference, 28.9%; 95% CI, 13.5% to 44.4%). Treatment-emergent adverse events occurred in 43.2% of patients in the combination group and 19.4% of patients in the single-arm. The most frequent treatment-emergent adverse events of grades 3 or higher were decreased neutrophil count (14.9% in combination group vs. 8.3% in PLD arm), hypertension (8.1% vs. none) and decreased white blood cell count (6.8% vs 4.2%). Overall, the addition of apatinib to PLD had increased clinical benefits with a manageable safety profile.
Image: PD
©2022 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.





{kind=link}