
Cardiovascular testing after emergency department presentation may not reduce risk of myocardial infarction
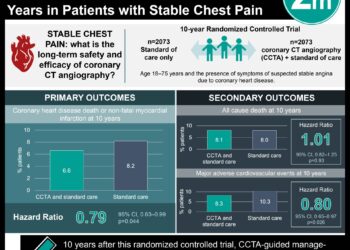
1. Based on this retrospective cohort study, noninvasive testing done within 30 days of patient presentation with chest pain at the emergency department reduced the amount of coronary angiography and revascularization done at 1 year.
2. Noninvasive testing, however, did not reduce risk of acute myocardial infarction admission at one year.
Evidence Rating Level: 2 (Good)
Study Rundown: Appropriate investigation of emergency department (ED) patients with chest pain but with negative findings of ischemia is important in order to reduce rates of acute myocardial infarction (AMI) and decrease rates of unnecessary testing. This retrospective cohort study aimed to determine whether noninvasive cardiovascular imaging or coronary angiography was associated with changes in rates of coronary revascularization or AMI admission in patients who present to the ED with chest pain but no findings of ischemia.
Patients who received cardiovascular testing had increased cardiovascular risk at baseline and greater risk of AMI admission at 30 days than those who did not receive testing. Noninvasive testing within 30 days of presentation was associated with an increase in coronary angiography and revascularization at one year however, no decrease in AMI admissions. Strengths of this study included its large size and comparison of weekday and weekend rates to ensure there was no selection bias. Limitations of this study included potential inability to generalize to those who are uninsured or older than 65 years old. Also, acute myocardial infarction admission rates were used as a surrogate for mortality. It is possible that mortality rates would be decreased with earlier screening where AMI rates would not change.
Click to read the study, published in JAMA Internal Medicine
Relevant Reading: Testing of Low-Risk Patients Presenting to the Emergency Department With Chest Pain: A Scientific Statement From the American Heart Association
In-Depth [retrospective cohort]: This large, retrospective cohort study was conducted from 2011 to 2012 using weekday and weekend national claims data from MarketScan Commercial Claims and Encounters. Data was divided into weekday and weekend information to account for differences in availability of cardiovascular testing. The study participants were privately insured adults aged 18 to 64 years that presented to the ED with chest pain without an initial diagnosis of acute myocardial ischemia. The exposures of interest were noninvasive testing or coronary angiography within 2 days or 30 days of ED presentation. Outcomes studied were coronary revascularization and admission for acute myocardial infarction at 7, 30, 180 and 365 days. Statistical analysis included multivariable logistic regression and adjusted for age, sex, hypertension, diabetes, dyslipidemia, ischemic heart disease, chronic kidney disease, cerebrovascular disease, peripheral vascular disease, tobacco use and presence of intervention in the preceding year.
A total of 926 633 privately insured patients were included in the cohort. As expected, those who presented on a weekday were more likely to receive cardiovascular testing than those who presented on a weekend. Of those who underwent testing, 91% had noninvasive testing. On adjusted analyses, patients who underwent cardiovascular testing within 2 or 30 days had higher rates of coronary angiography (36.5 per 1000 patients tested; 95%CI 21.0 to 52.0), revascularization (22.8 per 1000 patients tested; 95%CI 10.6 to 35.0) but no significant change in AMI admissions (7.8 per 1000 patients tested; 95%CI -1.4 to 17.0) at the end of follow-up of 365 days.
Image: PD
©2017 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.





{kind=link}