




{kind=link}


Ceftriaxone vs. norfloxacin for prophylaxis in patients with cirrhosis and gastrointestinal bleeding [Classics Series]
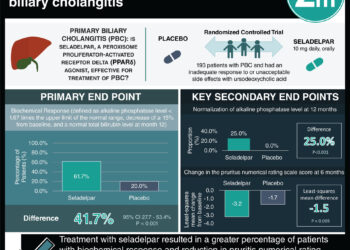
1. In cirrhotic patients who presented with gastrointestinal bleeding, patients treated with ceftriaxone were significantly less likely to develop proved or possible infections when compared to those treated with norfloxacin.
2. The ceftriaxone group was also significantly less likely to developed proved infections or spontaneous bacteremia and bacterial peritonitis.
3. There were no significant differences between the two groups in 10-day or hospital mortality.
Original Date of Publication: October 2006
Study Rundown: Patients with cirrhosis are at elevated risk of developing gastrointestinal bleeding. Cirrhotic patients who present with gastrointestinal bleeding are also at significant risk of bacterial infection, with large proportions of patients either presenting with bacterial infections or developing them during their hospitalization. Previous efforts had shown that antibiotic prophylaxis in these patients significantly reduced the risk of infection, though questions remained regarding the best antibiotic choice. While norfloxacin was commonly used, rising prevalence of quinolone resistance was rendering this less effective. The purpose of this trial was to compare the effects of oral norfloxacin with intravenous ceftriaxone when used in prophylaxis for cirrhotic patients presenting with gastrointestinal bleeding.
In summary, patients with cirrhosis presenting with gastrointestinal bleeding were significantly less likely to develop proved or possible infections when treated with ceftriaxone as compared with norfloxacin. Those on ceftriaxone were also significantly less likely to develop proved infections and spontaneous bacteremia or spontaneous bacterial peritonitis. There were no significant differences between the groups in 10-day or hospital mortality, and there were no drug-related adverse events noted during the study period.
Click to read the study in Gastroenterology
In-Depth [randomized controlled trial]: This randomized trial was conducted at 4 hospitals in Spain. Patients were included if they were between 18-80 years of age, had hematemesis and/or melena in the 24 hours prior to enrollment, and advanced cirrhosis (i.e., ≥2 of severe malnutrition, serum bilirubin >3 mg/mL, ascites, hepatic encephalopathy). Exclusion criteria were allergy to cephalosporin or quinolones, signs of infection (i.e., fever >37.5°C, white cell count >15 000/mm3, immature neutrophils >500/mm3, ascitic polymorphonuclear cell count >250/mm3, >15 leukocytes/field in urine sediment, pneumonia on chest x-ray), treatment with antibiotics 2 weeks before bleed, known advanced hepatocellular carcinoma, and human immunodeficiency virus infection. Eligible patients were randomized in a 1:1 ratio to norfloxacin 400 mg orally every 12 hours or ceftriaxone 1 g intravenously daily for 7 days. The primary outcome was the development of proved or possible infection in the 10 days after enrollment.
A total of 124 patients were randomized, with 111 being considered in the final analysis. Patients in the ceftriaxone group were significantly less likely to develop proved or possible infection when compared with those on norfloxacin (11% vs. 33%, p = 0.01). Patients in the ceftriaxone group were also significantly less likely to develop proved infection (11% vs. 26%, p = 0.03) or spontaneous bacteremia or bacterial peritonitis (2% vs. 12%, p = 0.03). There were no significant differences between the two groups in 10-day or hospital mortality. No adverse effects related to norfloxacin or ceftriaxone were observed during the study period.
Image: PD
©2015 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports
