
Cetuximab and bevacizumab are similar in combined platin therapy for advanced or metastatic colorectal cancer
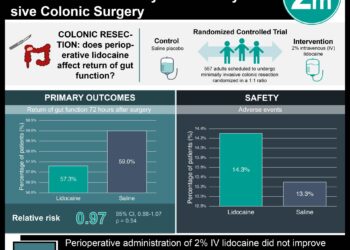
1. In this randomized controlled trial, cetuximab or bevacizumab combined with platin therapy had similar survival rates for patients with KRAS wildtype, advanced, or metastatic colorectal cancer.
2. Response rates and progression free survival were also equivocal for both groups of patients.
Evidence Rating Level: 1 (Excellent)
Study Rundown: Though platin therapy with either mFOLFOX6 or FOLFIRI remains the mainstay of treatment for advanced or metastatic colorectal cancer, some evidence suggests that the addition of certain monoclonal antibodies to these therapies may be more active for patients with KRAS wildtype tumors. Cetuximab, a chimeric EGFR monoclonal antibody, or bevacizumab, a humanized murine antihuman VGFR monoclonal antibody, have been approved as adjunct therapies with platins for advanced colorectal cancer. In this randomized controlled trial, either cetuximab or bevacizumab was randomly added to the patient’s choice of mFOLFOX6 or FOLFIRI therapy for KRAS wildtype colorectal cancer. There were no differences between the two groups for overall survival, progression free survival, nor in the rate of adverse events.
Click to read the study, published in JAMA
Relevant Reading: Bevacizumab in Combination With Oxaliplatin-Based Chemotherapy As First-Line Therapy in Metastatic Colorectal Cancer: A Randomized Phase III Study
In-Depth [randomized controlled trial]: A total of 1137 patients with advanced or metastatic, KRAS wildtype colorectal cancer were randomly assigned to either a cetuximab or bevacizumab plus mFOLFOX6/FOLFIRI platin therapies as part of the Cancer and Leukemia B and Southwest Oncology Group 80405 trial from September 2005 until September 2012. Eligible patients were without CNS metastasis or grade 2+ peripheral neuropathy, well controlled blood pressure, no congestive heart failure, no significant bleeding event within 6 months, no GI perforations within 12 months, less than 6 months of prior adjuvant therapy within the last 12 months, less than 5040 cGY of radiotherapy, and no major surgery within the last 4 weeks. 76.9% of patients died by the end of the study, and 82% experienced disease progression. No significant difference between cetuximab or bevacizumab were detected for median overall survival (HR 0.88; CI95 0.77 to 1.01), median progression-free survival (HR 0.95; CI95 0.84 to 1.08), or response rates (55.2% bevacizumab vs 59.6% cetuximab; chi-squared test with p = 0.13). Unplanned subgroup analyses by sex, race or chemotherapy subsets did not yield significant differences (p > 0.05), with the exception of a small difference in superiority for cetuximab over bevacizumab in the mFOLFOX6 subgroup (HR 0.83; CI95 0.71 to 0.98). There were no significant differences found for adverse events (p > 0.05).
Image: CC/Wiki
©2017 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.





{kind=link}