
Computed tomography findings may be useful in prognostication for mild traumatic brain injury
1. Computed tomography (CT) findings improved generalized estimating equation models predicting whether a patient would experience incomplete recovery or unfavorable outcome in mild traumatic brain injury.
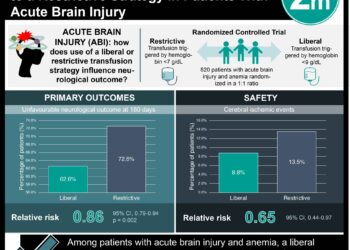
2. Patients with contusion, subarachnoid hemorrhage, and/or subdural hemorrhage were more likely than those with other radiologic findings on computed tomography (CT) to have incomplete recovery and unfavorable outcomes at a year. Patients with intraventricular hemorrhage or petechial hemorrhage had unfavorable outcomes at a year. Patients with epidural hemorrhage only had incomplete recovery early, but not at a year out from injury.
Evidence Rating Level: 2 (Good)
Study Rundown: Computed tomography (CT) is the gold-standard imaging for diagnosis of traumatic brain injury (TBI). Individual features on CT are not well understood as to how they predict prognosis of intracranial lesions from mild TBI (mTBI). Since the behavioural changes of mTBI are milder than severe TBI, it follows there are even subtler manifestations on imaging. This study aims to detect these subtle changes on imaging that can be useful in the prognosis of mTBI using a large observational cohort followed for 12 months post-mTBI. 64.2% of 1935 eligible adults with mTBI had head CT scans that were blindly assessed for acute intracranial abnormality. 37% of patients had a positive head CT, which were more frequent in men, patients with higher education who had no history of TBI, and were less common in Black individuals. Positive findings were most commonly subarachnoid hemorrhage (SAH), followed by subdural hematoma (SDH) and contusion. Patients with incomplete recovery, defined as a Glasgow Outcome Scale-Extended (GOSE) score of <8, were more commonly female, had neuropsychiatric history, TBI history, older age, or more education. Unfavorable outcomes, defined as a GOSE score of <5, were associated with older age and higher education. Patients with contusion, SAH, and/or SDH, were more likely to have incomplete recovery and unfavorable outcomes at a year. Patients with intraventricular hemorrhage (IVH) or petechial hemorrhage (PH) had unfavorable outcomes at a year. Patients with epidural hemorrhage (EDH) only had incomplete recovery early on post-injury. Estimation models of whether a patient would experience incomplete recovery or unfavorable outcomes improved when CT variables were added. Results remained consistent even when the worse GCS patients were removed from analysis, suggesting these are not reflective of severity of injury. These results were largely externally validated in the Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) study cohort. A limitation of this study includes that the follow-up rate of the TRACK-TBI cohort is low, at only 64.2% at 12 months. Patients that fail to follow-up might have differed in outcome from those who continue to follow-up. This is less likely, however, since the rate of positive CTs for those that followed-up for all 12 months is similar to that of those who followed-up at least once. The rates of hospitalization or intensive care unit admission were reported as higher in this study than others, which might be perceived as a limitation or flaw in the sampling or definition of mTBI, but would not affect the hierarchical cluster analysis or multiple correspondence analysis.
Click to read the study in JAMA Neurology
Relevant Reading: Advanced neuroimaging in traumatic brain injury: an overview
In-Depth [prospective cohort]: Patients for this study were a subset of those from the Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) study. Adult patients (17+) presenting at 1 of 18 US level 1 trauma centers with mTBI (GCS 13 to 15) occurring in the previous 24 hours who had indication for a head CT were eligible. Patients were excluded if they were pregnant, incarcerated, had non-survivable physical trauma, or had preexisting medical or neuropsychiatric conditions. All patient CT scans were blindly assessed for imaging features, where a positive CT was defined as the presence of any acute intracranial abnormality. The CENTER-TBI study cohort, which had largely similar results to this study, was used as an external validation set. The TRACK-TBI cohort had 1935 eligible individuals (66.5% men), 64.2% of whom had outcome measured available at 12 months. Most patients were hospitalized without intensive care unit stay (43.0%). Positive head CTs occurred more in men than women (39.2% vs 32.5%, P = 0.004), individuals with higher education levels (13.6±3.2 years vs 13.4±2.7 years, P = 0.046), and those without a history of TBI compared to those with (26.0% vs 34.8%, P < 0.001), and less in Black individuals (23.3% vs 39.7%; P<0.001). 37.0% of patients had a positive CT result for acute intracranial pathology, which mostly consisted of subarachnoid hemorrhage (22.0%), subdural hematoma (SDH) with contusion (12.9%), SDH (11.9%), or SAH with SDH (10.2%). The Patients with incomplete recovery more commonly were female (1.73 [95% CI, 1.43-2.08]; P < 0.001), had neuropsychiatric history (1.61 [95% CI, 1.31-1.99]; P < 0.001), TBI history (1.39 [95% CI, 1.16-1.67]; P < 0.001), age >55 (OR, 1.17 [95% CI, 1.00-1.37]; P = 0.04), or more education (0.64 [95% CI, 0.57-0.74]; P < 0.001). Unfavorable outcomes were similarly associated with age >55 (2.64 [95% CI, 2.02-3.46]; P < 0.001) and higher education (0.60 [95% CI, 0.47-0.76]; P < 0.001). Hierarchical cluster analysis classified mTBI patients as: Group 1: contusion, SAH, and/or SDH, Group 2: IVH or PH, or Group 3: EDH. Group 1 Contusion, SAH, and/or SDH patients were more likely to have incomplete recovery at 6 months (1.67 [95% CI, 1.28-2.17]) and more unfavorable outcomes at a year (3.23 [95% CI, 1.59-6.58]). Group 2 IVH or PH patients also had unfavorable outcomes through month 12 (3.47 [95% CI, 1.66-7.26]). Group 3 EDH patients only had incomplete recovery early in recovery, up to 3 months (2.33 [95% CI, 1.28-4.24], P = 0.006). Marginal R2 of generalized estimating equation models improved with CT variables compared to without for incomplete recovery (11.2% vs 9.1%) and unfavorable outcomes (10.0% vs 7.8%) identification. Incomplete recovery until 6 months was associated with isolated SAH (1.57 [95% CI, 1.01-2.43]). Since worse GCS scores might indicate worse prognosis, these results were analyzed again without participants with a GCS of 13 and found to remain.
Image: PD
©2021 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.




{kind=link}