
Delayed denosumab doses associated with increased the risk of vertebral fractures
1. Delayed subsequent denosumab doses were shown to increase the risk for vertebral fractures compared to on-time injection.
2. There was insufficient evidence to determine if with delayed dosing, fracture risk at other locations would be increased.
Evidence Rating Level: 2 (Good)
Study Rundown: Denosumab, a monoclonal antibody that inhibits the RANK ligand on osteoblasts, is an effective treatment for osteoporosis. Discontinuation of the therapy results in accelerated bone turnover and rapid loss of bone mineral density. Furthermore, cessation of denosumab has been associated with an increased risk of vertebral and hip fractures. However, the effect of delayed subsequent denosumab doses on fractures risks is yet to be determined. As such, this study examined the effect of denosumab delay on fracture risk. The study concluded that delayed denosumab doses only increased the risk for vertebral fractures and not fractures at other anatomical sites. This retrospective cohort study was limited by statistical power for composite fracture and several secondary end points. Therefore, the data was not sufficient to conclude the risk of fractures at other anatomical sites was caused by a delayed denosumab dosing regimen. Nonetheless, this study was strengthened by the adoption of a target trial emulation design, which aligned the results from the study with those from randomized control trials since a randomized control trial within this patient population would be considered unethical.
Click to read the study in Annals of Internal Medicine
Relevant Reading: Vertebral fractures after discontinuation of denosumab: a post hoc analysis of the randomized placebo-controlled FREEDOM trial and its extension
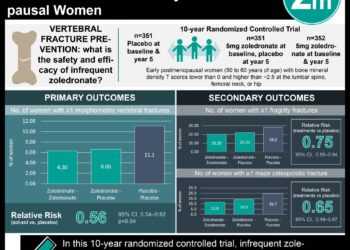
In-Depth [retrospective cohort]: This retrospective, cohort study enrolled 2594 patients through The Health Improvement Network (THIN) database in the United Kingdom. Participants were included if they met the criteria of 45 years or older with an initiated denosumab treatment to manage osteoporosis between 2010 and 2019. Participants that received only 1 denosumab injection or used other antiosteoporosis drugs were excluded from the study. The recommended date for a subsequent denosumab dose was set to 6 months after a prior dose. The administration of a subsequent dose within 4 weeks was classified as “on-time”, a dose administered between 4 and 16 weeks was considered “short delay”, and a dose given at 6 months was classified as “long delay”. The primary outcome was composite fractures, which included all types of fractures. The secondary outcomes were osteoporotic fractures, which included vertebral fractures, hip fractures, and nonvertebral fractures. Over the 6-month period, the cumulative risk for composite fractures for the 3 groups was 27.3 in 1000 for “on-time”, 32.2 in 1000 for “short delay”, and 42.4 in 1000 for “long delay”. The risk difference between “short delay” and “on-time” dosing was 4.8 in 1000 (hazard ratio, 1.03, 95% confidence interval [CI], 0.63 to 1.69) compared to the risk difference between “long delay” and “on-time” dosing, which was 15.0 in 1000 (hazard ratio, 1.44, 95% CI, 0.96 to 2.17, P=0.093). Specifically focusing on vertebral fractures, the cumulative risk was 2.2 in 1000 for “on-time”, 3.6 in 1000 for “short delay”, and 10.1 in 1000 for “long delay”. The risk difference between “short delay” and “on-time” dosing was 1.4 in 1000 (hazard ratio, 1.48, 95% CI, 0.58 to 3.79) compared to the risk difference between “long delay” and “on-time” dosing, which was 7.9 in 1000 (hazard ratio, 3.91, 95% CI 1.62 to 9.45, P=0.005). Taken together, delaying subsequent denosumab doses increased the risk for composite fractures, especially vertebral fractures.
Image: PD
©2020 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.




{kind=link}