




{kind=link}


Diagnosis of attention-deficit/hyperactivity disorder associated with severe traumatic brain injury in children
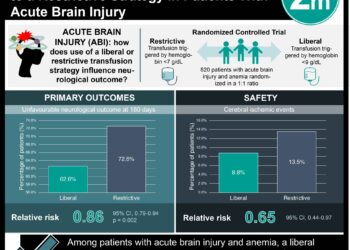
1. A meta-analysis including over 12,000 pediatric patients found that the diagnosis of attention-deficit/hyperactivity disorder (ADHD) was significantly associated with a history of severe, but not mild or moderate, traumatic brain injury (TBI).
2. More than one third of children who had suffered a severe TBI had been diagnosed with ADHD up to one year post-injury.
Evidence Rating: 1 (Excellent)
Study Rundown: The long-term consequences of traumatic brain injury (TBI) are poorly understood, particularly in the pediatric population. Asarnow et al conducted a systematic review & meta-analysis to understand the relationship between attention-deficit/hyperactivity disorder (ADHD) and TBI in children aged 4-18. Three large databases were systematically searched from 1981 through to 2020. The authors extracted information about the severity of injury & patient ADHD-status before and after injury, following them up to a year after TBI. 24 studies with a total of 12,374 individual patients were found to be eligible for inclusion. Patients diagnosed with ADHD prior to TBI event were not included in the analysis. TBI patients were subdivided on the basis of injury severity and were compared to healthy controls and to controls with other, non-TBI injuries. There was no significant difference in pre-injury rates of ADHD diagnosis between children who had experienced mild, moderate or severe TBI. Interestingly, the rate of pre-injury ADHD in the TBI group regardless of severity was significantly higher than in both control groups. Children with severe TBI were at higher odds of being diagnosed with ADHD compared to both injured and non-injured controls at all time points assessed following injury. The meta-analysis found that 35.5% of severe TBI children were diagnosed with ADHD at the one year post-injury time point. Asarnow et al.’s analysis is the first large meta-analysis of studies examining the relationship between TBI and ADHD. The longitudinal timeline (over one year) and large sample size certainly lend fortitude to the results reported here. Additionally, the high incidence of ADHD following severe TBI in this study is shocking and may contribute to the important discussion of pediatric head protection and safety in sports. There are some methodological shortcomings of this study; there was some clinical heterogeneity amongst the studies included, namely with regards to the criteria used to diagnose ADHD. Unclear diagnostic criteria raises the question as to whether ADHD was more likely to be diagnosed in the severe TBI group simply because they received more close medical attention over time, or because their history of TBI lends itself more easily to an ADHD diagnosis. The systematic review/meta-analysis does not allow for confounders to be controlled for. Finally, a variety of study designs were included, each with their intrinsic biases and variable study quality. It is important that these results be interpreted in the context of an individual patient when applied clinically.
Click to read the study in JAMA Pediatrics
Click to read an accompanying editorial in JAMA
Relevant Reading: Epidemiology and outcomes of pediatric traumatic brain injury
In Depth [systematic review and meta-analysis]: Search criteria for this study are described in the manuscript; the search was limited to studies published in peer-reviewed journals in the English language. Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines were adhered to. Study selection was completed independently by at least two of three authors, as was rating of study quality using the Newcastle-Ottawa scale. Outcomes of interest were pre-defined and extracted using standardized methodology. A Bayesian random-effects model was used for data analysis. Results were reported using the Odds Ratio (OR) and 95% confidence intervals (CI). The OR for ADHD after severe TBI within one year was 2.62 (95% CI 0.76-6.64), and after one year the OR was 6.25 (95% CI 2.06-15.06) compared to non-injured controls.
Image: PD
©2021 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports
