
Disposable elevator cap duodenoscopes may reduce contamination in endoscopic retrograde cholangiopancreatography – the ICECAP trial
1. Duodenal contamination was detected in 11.2% of patients who underwent endoscopic retrograde cholangiopancreatography (ERCP) using a standard duodenoscope and 3.8% of patients using a disposable elevator cap duodenoscope.
2. Both scopes were sufficient in acquiring the same level of technical success.
Level of Evidence Rating: 1 (Excellent)
Study Rundown: Endoscopic retrograde cholangiopancreatography (ERCP) is a critical tool in the management of conditions of the pancreas and biliary tree. Given the invasive nature of this procedure, it is possible that bacterial contamination may take place. This is combated with stringent methods of cleaning equipment, including duodenoscopes. Several new designs for duodenoscopes have been developed in recent years, including those with disposable elevator caps, which may reduce the potential for contamination. The present study sought to evaluate the utility of disposable elevator cap duodenoscopes in reducing contamination and maintaining strong technical performance in comparison to standard duodenoscopes.
518 patients in total were recruited in this study between 2019 and 2022, including 529 patients in the disposable cap group and 529 patients in the standard duodenoscope group. 11.2% of scopes in the standard duodenoscope group had evidence of persistent bacterial contamination, while only 3.8% of the disposable cap scopes did. Rates of technical success were equivalent between the two groups (94.6% vs. 90.7%). There were no significant differences in patient tolerability or reported discomfort, nausea and abdominal distention between the two groups. Finally, there were no significant differences in adverse outcomes, including ascending cholangitis, pancreatitis, bleeding, perforation and 30-day mortality between the experimental and control groups.
Forbes et al demonstrated equivalent technical and clinical outcomes between the disposable cap and standard duodenoscopes in performing ERCPs amongst Canadian adults, although rates of instrument bacterial colonization were significantly lower with disposable scopes. Strengths of this trial included the large number of patients and the randomized design, which does well to control for confounding variables. Interpretation of this study should be cognizant that these results are specific to the local microbial profile at two select healthcare centers, and therefore, external validity is limited.
Click here to read this study in JAMA Internal Medicine
Click to read an accompanying editorial in JAMA Internal Medicine
Relevant reading: Endoscopic retrograde cholangiopancreatography-related complications and their management: a “scoping” literature review
In-Depth [randomized controlled trial]: The Infection Control in ERCP using a Duodenoscope with a Disposable Cap (ICECAP) study was a randomized, controlled trial conducted in two Canadian centers. Eligible patients were adults undergoing ERCP who were able to complete 30-day follow-up. Randomization was done through a computer-based system in a 1:1 fashion. The two outcomes of interest were (1) measures of bacterial contamination following scope cleaning (>10 colony-forming units of bacteria or gram-negative bacterial growth within 72 hours) and (2) technical success of ERCP (determined by two, independent and blinded adjudicators based on a priori) criteria. Standardized protocols were followed for the deployment of scopes and sterilization.
Significantly more persistent bacterial contamination was present in the standard duodenoscope group than in the disposable cap group (11.2% vs. 3.8%). The relative risk of bacterial contamination was 0.34 (95% confidence interval 0.16-0.75) in favour of the experimental group. The technical success rate was considered non-inferior in the experimental group (90.7%) versus the control group (94.6%) (p=0.13). Rates for secondary outcomes were not significantly different between the two groups: cholangitis (0.8% vs 1.2%, P > .99), pancreatitis (3.1% vs 3.5%, P > .99), bleeding (1.9% vs 1.2%, P = .72), perforation (0.4% vs 0.0%, P > .99) and 30-day mortality (0.4% vs 0.4%, P > .99).
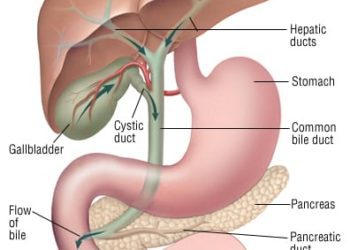
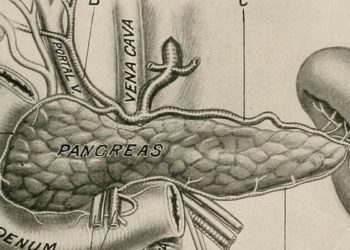
Image: PD
©2023 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.




{kind=link}