



{kind=link}


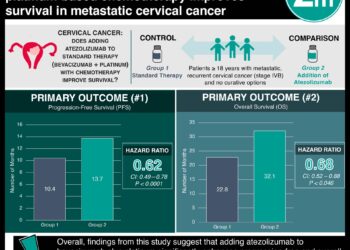
First line bevacizumab fails to improve survival newly diagnosed glioblastoma patients [AVAglio trial]
Image: PD
1. Bevacizumab as a first-line agent alongside temozolomide and radiotherapy increased progression-free survival, but did not increase overall survival.
2. Bevacizumab incorporation was associated with an improved quality of life, but also a higher rate of serious adverse events.
Evidence Rating Level: 1 (Excellent)
Study Rundown: Glioblastoma is a primary brain cancer which, when progressive, leads to neurocognitive debilitation and death. The standard therapy for newly diagnosed glioblastoma is surgical resection, followed by radiation and chemotherapy with temozolomide.
Bevacizumab (Avastin, Genetech/Roche) is a monoclonal antibody against VEGF, an angiogenic factor that is overexpressed by glioblastoma tumors. In 2009, bevacizumab was approved by the FDA for treatment of recurrent glioblastoma.
This phase 3 trial, sponsored by Roche and known as AVAglio, investigated the use of bevacizumab as a first-line agent against glioblastoma, alongside radiation and temozolomide. The study found that the incorporation of bevacizumab improved progression free-survival and preserved quality of life, but did not increase overall survival. Additionally, bevacizumab was associated with a greater rate of serious adverse events, mostly bleeding, hypertension and proteinuria.
Although bevacizumab did not increase overall survival, progression-free survival with preserved quality of life and functional status are important outcomes. This benefit may outweigh the increased risk of adverse events. However, this trial’s results must be compared to those of the RTOG 0825 trial, a similar trial published in the same issue of NEJM which found that functional status and quality of life were not improved with bevacizumab.
Click to read the study in NEJM
Click to read an accompanying editorial in the NEJM
Relevant Reading: A Randomized Trial of Bevacizumab for Newly Diagnosed Glioblastoma
In-Depth [randomized, double-blind, placebo-controlled trial]: This trial enrolled a total of 921 patients. All patients were enrolled within about a month of surgery and randomized to radiation with temozolomide plus either bevacizumab or placebo. This was followed by a 28-day treatment break, followed by a maintenance regimen of temozolomide plus either bevacizumab or placebo for six 4-week cycles. Finally, there was a monotherapy phase of either bevacizumab or placebo every 3 weeks.
The bevacizumab group had an increase in median progression-free survival of about 4 months (10.6 months vs. 6.2 months; P<0.001). It should be noted that part of the assessment for tumor-progression included MRI. By altering vascular permeability within tumors, bevacizumab may alter the appearance of tumors on MRI, and thereby conceal progression. However, the preservation of functional status in the bevacizumab group argues that there was a real effect in delaying progression.
The overall survival was similar between the bevacizumab and placebo groups (33.9% and 30.1% at 2 years; P=0.24). More patients on bevacizumab experienced adverse events grade 3 or higher (66.8% vs. 51.3%; P<0.001).
More from this author: Early risk factor for progression of cystic fibrosis identified, Gut microbes implicated in stroke and heart attacks: new dietary link, New leukemia mutation offers therapeutic targets, Childhood ADHD associated with increased risk of suicide, A marker of aggressive liver cancer and potential therapeutic target identified
©2012-2014 2minutemedicine.com. All rights reserved. No works may be reproduced without expressed written consent from 2minutemedicine.com. Disclaimer: We present factual information directly from peer reviewed medical journals. No post should be construed as medical advice and is not intended as such by the authors, editors, staff or by 2minutemedicine.com. PLEASE SEE A HEALTHCARE PROVIDER IN YOUR AREA IF YOU SEEK MEDICAL ADVICE OF ANY SORT.
RelatedReports
