






In early STEMI patients, prehospital fibrinolysis is non-inferior to PCI
[tabs tab1=”2MM Rundown” tab2= “2MM Full Report”]
[tab]
Image: CC/JHeauser
1. For early STEMI patients who could not undergo timely PCI within 1 hour, prehospital fibrinolysis coupled with coronary angiography was non-inferior to PCI.
2. Fibrinolytic therapy was associated with an increased risk of stroke and intracranial hemorrhage.
This multi-center randomized control study randomized patients with early STEMI who could not receive PCI within 1 hour of symptom onset, to prehospital fibrinolysis with early coronary angiography, or PCI. There was no difference in the primary endpoint, but there was an increased risk of stroke and intracranial hemorrhage in patients who had received fibrinolysis treatment. The standard of care is for patients with STEMI to receive PCI within 1 hour of symptoms. Although many studies have shown PCI to be superior to fibrinolysis, fibrinolysis continues to be used for reperfusion, largely due to lack of access to primary PCI. This study suggests that fibrinolysis continues to be a suitable alternative to PCI if a PCI-capable hospital cannot be reached within an hour.
As this was a multi-center trial that included elderly patients, the results are generalizable. One major limitation is that the study was not adequately powered to demonstrate how different age groups were affected by fibrinolysis vs. PCI. Also, the follow-up time was short, and whether the outcomes are similar in the long term remains unknown. Another limitation of this study is that much of PCI technology has advanced since this study was concluded: drug-eluting stents have become much safer and have a much lower risk of thrombosis. Future studies will need to determine whether prehospital fibrinolysis coupled with timely coronary angiography is still non-inferior to the new generation of PCI technology in patients who could not receive PCI within one hour of symptom onset.
Click to read the study in NEJM
Click to read an accompanying editorial in NEJM
[/tab]
[tab]
Image: CC/JHeauser
1. For early STEMI patients who could not undergo timely PCI within 1 hour, prehospital fibrinolysis coupled with coronary angiography was non-inferior to PCI.
2. Fibrinolytic therapy was associated with an increased risk of stroke and intracranial hemorrhage.
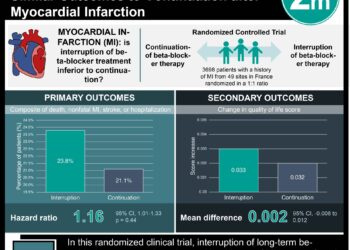
This [randomized controlled] study: compared outcomes of 1892 patients who presented to a hospital with an early acute ST-elevation myocardial infarction (STEMI) and who could not receive PCI within the first hour of symptoms. Patients were randomized to either percutaneous coronary intervention (PCI) or prehospital fibrinolysis with tenecteplase, clopidogrel and enoxaparin followed by timely coronary angiography. The primary endpoint was a composite of 30-day all-cause mortality, shock, congestive heart failure, or reinfarction.
The incidence of the primary endpoint was not significantly different in patients who received prehospital fibrinolysis vs. those who received PCI (12.4% vs. 14.3%, p=0.21). However, there was an increase in the number of strokes and intracranial hemorrhages in those that received fibrinolysis (1% vs. 0.2%, p=0.04), higher in the elderly population. Decreasing the dosage of fibrinolytics by half for elderly patients eliminated any differences in the risk of intracranial hemorrhages.
In sum: This multi-center randomized control study randomized patients with early STEMI who could not receive PCI within 1 hour of symptom onset, to prehospital fibrinolysis with early coronary angiography, or PCI. There was no difference in the primary endpoint, but there was an increased risk of stroke and intracranial hemorrhage in patients who had received fibrinolysis treatment. The standard of care is for patients with STEMI to receive PCI within 1 hour of symptoms. Although many studies have shown PCI to be superior to fibrinolysis, fibrinolysis continues to be used for reperfusion, largely due to lack of access to primary PCI. This study suggests that fibrinolysis continues to be a suitable alternative to PCI if a PCI-capable hospital cannot be reached within an hour.
As this was a multi-center trial that included elderly patients, the results are generalizable. One major limitation is that the study was not adequately powered to demonstrate how different age groups were affected by fibrinolysis vs. PCI. Also, the follow-up time was short, and whether the outcomes are similar in the long term remains unknown. Another limitation of this study is that much of PCI technology has advanced since this study was concluded: drug-eluting stents have become much safer and have a much lower risk of thrombosis. Future studies will need to determine whether prehospital fibrinolysis coupled with timely coronary angiography is still non-inferior to the new generation of PCI technology in patients who could not receive PCI within one hour of symptom onset.
Click to read the study in NEJM
Click to read an accompanying editorial in NEJM
By Jeremy Chan and Mitalee Patil
More from this author: Artifical pancreas lowers the risk of overnight hypoglycemia in children, Selumetinib increases the uptake of radioiodine in patients with metastatic thyroid cancer refractory to radioiodine
© 2013 2minutemedicine.com. All rights reserved. No works may be reproduced without written consent from 2minutemedicine.com. Disclaimer: We present factual information directly from peer reviewed medical journals. No post should be construed as medical advice and is not intended as such by the authors or by 2minutemedicine.com. PLEASE SEE A HEALTHCARE PROVIDER IN YOUR AREA IF YOU SEEK MEDICAL ADVICE OF ANY SORT. Content is produced in accordance with fair use copyrights solely and strictly for the purpose of teaching, news and criticism. No benefit, monetary or otherwise, is realized by any participants or the owner of this domain.
[/tab]
[/tabs]
RelatedReports
