
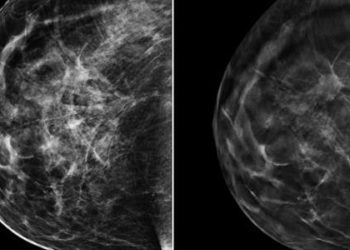
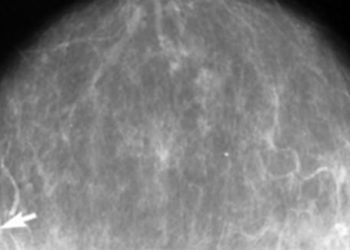
MRI assessment of breast parenchymal enhancement may predict cancer risk
1. In women at high risk for breast cancer, screening magnetic resonance imaging was used to qualitatively assess the degree of background parenchymal enhancement and was found to be associated with a 9-fold increase in risk for the development of breast cancer within roughly 5 years of the index study.
2. Any degree of background parenchymal enhancement beyond baseline was associated with an increased risk of breast cancer development, however mammographic breast density and the extent of fibroglandular breast tissue were not associated with any change in baseline breast cancer risk.
Evidence Rating Level: 2 (Good)
Study Rundown: Breast magnetic resonance imaging (MRI) uses magnetic fields to create detailed images of soft tissue anatomy within the breast and has been suggested as an adjunct to mammography and ultrasound imaging in cancer screening. Although breast MRI is not currently part of the standard screening regimen, it may help detect breast cancer in its earliest stage for some women who are at high risk for developing the disease by screening for imaging biomarkers that predict oncogenesis. In women at high risk secondary to a strong family history or the presence of certain genetic mutations such as the BRCA gene, MRI may provide a useful adjunct in its ability to assess breast density, the degree of fibroglandular tissue within the breast and the level of background contrast material-enhancement which may correlate to increased hormone responsive tissue, neovascularity or vascular permeability, theoretical markers of breast cancer physiology. The current study retrospectively examined screening breast MRIs from high-risk women 18 years or older with no prior diagnosis of breast cancer and individually compared the degree of background parenchymal enhancement (BPE), mammographic breast density, and fibroglandular tissue on MR to the incidence of breast cancer diagnoses during follow-up.
Compared to patients with minimal or no BPE on MRI, those with elevated BPE were found to be 9 times more likely to develop breast cancer during the study follow-up interval, suggesting that BPE may be a potent biomarker in breast cancer screening among high risk patients, and may be qualitatively assessed on screening MRI. In contrast, mammographic breast density and the amount of fibroglandular tissue appeared to have no significant relationship to cancer risk in the study group. Additionally, despite the fact that BPE levels are associated with the level of circulating estrogen, there was no association between increased BPE and estrogen receptor positivity in the subsequent breast cancer diagnoses within the cohort, suggesting that BPE may be a generalizable biomarker of tumorigenesis. This study was limited in that it relied on qualitative assessments of BPE without quantitative measures to limit inter- and intraobserver variability, and in that the MR imaging technique was altered during the course of the study. Additionally, the study suffered from a limited sample size leading to a lack of statistical power and potential concerns regarding generalizability. Additional, multicenter studies with larger study groups, lengthier follow-up intervals and cohorts matched across the range of baseline risk of breast cancer development would be helpful in characterizing the validity of BPE as a general risk predictor for breast cancer development.
Click to read the study in Radiology
Relevant Reading: Using clinical factors and mammographic breast density to estimate breast cancer risk: development and validation of a new predictive model.
In-Depth [retrospective cohort]: Medical records from 487 women aged 18 years or older, with an average age of 47 ± 10 years, who underwent MRI screening for breast cancer at a single institution between 2006 and 2011 were retrospectively reviewed. Only women at high risk for breast cancer without a prior diagnosis of breast cancer were included in the study, and were subsequently excluded if subject’s histories did not fit the American Cancer Society’s definition of high risk based on factors such as family history, or individual genetics. MRI features were assessed qualitatively for the degree of BPE (none, minimal, mild, moderate, and severe) and BPE pattern, and the extent of fibroglandular tissue, while breast density was assessed mammographically. Notably, the MRI technique varied over the course of the study due to evolution in standard practice and technology availability, with the largest change being a transition from a 1.5T scanner to 3.0T scanner roughly halfway through the study. During the mean follow-up period of 5.6 ± 1.3 years, 23 women were diagnosed with breast cancer, 6 of whom were BRCA positive, with a total of 12 invasive ductal carcinomas and 11 ductal carcinomas in situ (DCIS) diagnosed. One-to-one matching of age and BRCA status from this group to controls who did not develop breast cancer was performed for the study controls. Using conditional logistic regression, the results demonstrated that women with at least mild background parenchymal enhancement were nine times more likely to develop the disease than those without the MRI finding (p = 0.007; odds ratio = 9.0; 95% CI: 1.1, 71.0). However, no significant associations were found between disease risk and imaging features of BPE pattern (p = 0.5), amount of FGT (p = 0.5), and breast density on mammography (p = 0.4).
Image: PD
©2015 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.




{kind=link}