
Organ Transplant-Associated Immunosuppression and Cutaneous Squamous Cell Carcinoma Outcomes
1. In this Norwegian study, patients receiving organ transplants with cutaneous squamous cell carcinoma (cSCC) had higher rates of developing a second cSCC, metastasis, and death from cSCC when compared to patients with cSCC not receiving organ transplants.
2. In order to ensure proper follow-up and skin cancer care policies, clinicians should be aware of the increased risk of second cSCC, metastasis, and death for organ transplant-receiving patients with cSCC.
Evidence Rating Level: 2 (Good)
Study Rundown: Cutaneous squamous cell carcinoma (cSCC) is the second most common form of skin cancer. Metastasis risk for cSCC varies; higher risk has been linked to organ transplant recipients (OTRs) compared to immunocompetent patients. Therefore, this retrospective cohort study investigated cSCC recurrence, metastasis, and death in non-OTRs and OTRs. OTRs with cSCC resulted in higher rates for all outcomes than non-OTRs with cSCC. Limitations of this study included surveillance, potential misclassification of cancer-specific deaths, and the inability to distinguish between immunosuppression due to diseases or treatment unrelated to organ transplants. Furthermore, information on organ transplant type, immunosuppressive treatment regimen, and race and ethnicity were not collected. Strengths include its population-based design and reliable data spanning more than five decades.
Click to read the study in JAMA Dermatology
Relevant Reading: Analysis of risk factors determining the prognosis of cutaneous squamous-cell carcinoma: a prospective study
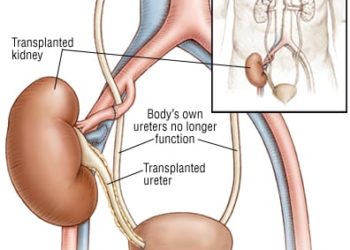
In-Depth [retrospective cohort]: The data for this nationwide retrospective cohort study was derived from the Cancer Registry of Norway from 47,992 patients diagnosed with cSCC at a minimum age of 18 across five decades (i.e., January 1, 1968, and December 31, 2020). Exclusion criteria included in-situ tumours and patients who had cSCC before their first organ transplant. The primary anatomic location of the tumours was categorized as ear, head and face (including eyelid), neck and trunk, perineum and perianal, upper limbs, lower limbs, multiple locations (>1 tumour within four months), and unspecified. A total of 8,278 patients received a kidney (75%), heart, lung, or liver transplant. Transplants occurred at the Oslo University Hospital between 1968 and 2012, followed by long-term immunosuppressive treatment. The primary outcomes were second cSCC, metastasis, and death from cSCC. In total, 1,208 OTRs (median age, 66 years [range, 27-89 years]; 882 men [73.0%] and 326 women [27.0%]) and 46,784 non-OTRs (median age, 79 years [range, 18-106 years]; 25 406 men [54.3%] and 21 378 women [45.7%]) were included. In OTRs, the second cSCC and metastasis rate per 1000 person-years was 250.6 (95% CI, 232.2-270.1) and 4.8 (95% CI, 3.4-6.7), respectively. In non-OTRs, the second cSCC and metastasis rate per 1000 person-years was 30.9 (95% CI, 30.2-31.6) and 2.8 (95% CI, 2.6-3.0), respectively. OTRs had a 4.3 and 1.5-fold increased rate for developing a second cSCC and metastasis, respectively. More deaths from cSCC occurred in OTRs (3.3%) compared to non-OTRs (1.1%). The death rate per 1000 person-years was 5.4 (95% CI, 3.9-7.4) and 1.7 (95% CI, 1.5-1.8) in OTRs and non-OTRs, respectively. OTRs had a 5.5-fold increased rate of death. Overall, rates of second cSCC, metastasis, and death from cSCC were significantly higher for OTRs with cSCC than non-OTRs with cSCC. However, most deaths in both groups were due to causes outside of cSCC.
Image: PD
©2023 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.




{kind=link}