

Patient Basics: Colon Polyps
Originally published by Harvard Health.
What Is It?
Colon polyps are growths of tissue inside the large intestine, also called the colon. Some polyps are mushroom-shaped protrusions on the end of a stalk. Others appear as bumps that lie flat against the intestinal wall.
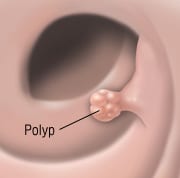
There are several types of polyps. Most are noncancerous (benign), but one type, the adenomatous polyp, is associated with changes (called mutations) in the DNA of the lining of the colon. These mutations can progress into colon cancer. The larger the polyp, the greater the chance that it contains cancerous cells.
Some people are born with a genetic tendency to develop multiple polyps. Inherited conditions such as familial adenomatous polyposis and Gardner’s syndrome can cause hundreds of polyps to grow in the colon and rectum. Without surgery to remove the affected section of the intestine, it is almost certain that at least one of these polyps will turn into cancer by middle age. These two conditions are rare.
Symptoms
Many times, people are not aware they have colon polyps because there are no symptoms. Larger growths can bleed, causing blood in the stool. Sometimes bleeding polyps can cause fatigue and other symptoms of anemia (low levels of red blood cells). On rare occasions, a large polyp can cause diarrhea or secretion of large amounts of potassium. This can cause marked fatigue and muscle weakness.
Diagnosis
Your doctor may use one or more of the following tests to determine whether you have colon polyps:
- Digital rectal exam — The doctor inserts a gloved finger into the rectum to check for unusual growths or formations. This can only detect polyps in the rectum, the lower few inches of the bowel.
- Fecal occult blood test — A sample of stool is examined for tiny traces of blood, an indication of polyps.
- Sigmoidoscopy — A thin, lighted tube fitted with a video camera is inserted into the colon through the rectum, allowing the doctor to examine the area for polyps. Small polyps can be removed through the scope.
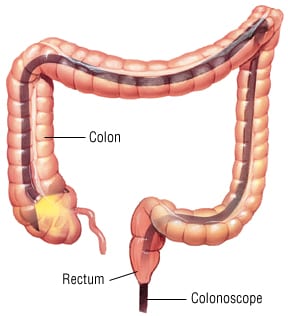
- Colonoscopy — A longer version of the instrument used in sigmoidoscopy is used to see the entire length of the colon. This is the only test that examines all the areas where cancers may grow. Small polyps can be removed through the scope.
- Barium enema — Chalky liquid is injected into the colon through the rectum, and then X-ray images are taken of the intestine. Air is usually inserted to expand the colon, making it easier to see if polyps are present.
- Virtual colonoscopy — similar to a barium enema; but instead of standard x-rays, a CT (computerized tomogram) scan is performed. These pictures give much better detail than what can be seen with a regular barium enema.
Expected Duration
If a polyp is not removed, it will continue to grow larger. It usually takes several years for a polyp to change to a cancer. However, some polyps have malignant cells even though they are small. About one-third of adenomatous polyps will progress to cancer in three to five years if undetected or ignored.
Prevention
The danger from polyps is that most cases of colon cancer spring from these growths. You can lower your chances of developing cancerous polyps in the following ways:
- Increase your consumption of fruits, vegetables and whole grains.
- Limit your intake of processed red meats.
- Get at least 30 minutes of physical exercise on most days.
- Maintain a healthy weight. Extra fat, especially around the waist alters your metabolism and increases your chances of developing colon and rectal cancer.
In addition, some research suggests these measures may help decrease the risk of colon cancer:
- A multivitamin or a vitamin D supplement daily — People who have a higher intake of vitamin D have a reduced risk of colon cancer compared to those with inadequate vitamin D intake.
- Taking aspirin-like drugs — In several studies, people who used aspirin or other non-steroidal anti-inflammatory drugs (NSAIDs) on a regular basis had a 40% to 50% lower chance of developing adenomatous polyps or colorectal cancer. Because of side effects of these drugs, taking them every day just to prevent colon cancer is not advised if your cancer risk is only average.
- Not smoking — Smoking increases the risk of colon cancer.
Women who take hormones after menopause have a lower risk of colon cancer. However, long term use of estrogen and progesterone after menopause should not be used for this purpose.
Because the risk of colon cancer increases with age, people age 50 and older should have periodic screening for early detection of polyps and colon cancer. Options for screening include:
- Colonoscopy — If normal, repeat in 10 years.
- Fecal occult blood testing yearly — An easy to perform test done at home.
- Flexible sigmoidoscopy every five years — Combined with yearly fecal occult blood testing.
- Double contrast barium enema — Use of this as a screening test has declined over the past decade.
- Virtual colonoscopy — Still requires the same type of colon preparation used before colonoscopy.
If you have a hereditary condition that causes polyps to overgrow in the large intestine, you should begin frequent examinations at puberty. Your doctor may advise complete removal of the colon because there is a high likelihood of developing colon cancer by age 40. The other option is frequent screening with colonoscopy. How often you will need to have this done depends upon your age and what was seen on your last colonoscopy.
Treatment
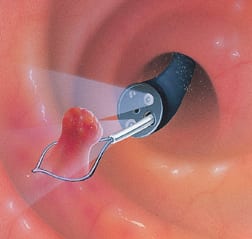
Often, the doctor can remove polyps during a colonoscopy. This is done by cutting the polyp from the wall of the colon using an electrical current passed through a wire loop at the end of the colonoscope. Sometimes, open surgery through the abdomen is necessary to remove a very large polyp. For cancerous polyps, surrounding tissue or a section of the colon may be removed as well.
When To Call A Professional
You should call immediately for advice if you develop rectal bleeding. You also should have routine colon examinations starting at age 50. People with a family history of colon cancer at an early age, familial adenomatous polyposis, or Gardner’s syndrome should begin screening earlier.
Prognosis
Polyps are common. But less than 1% of all polyps ever become cancerous. By removing polyps, the risk is even lower. Survival depends on the stage of cancer. If the cancerous cells are confined to a polyp or they have not grown deep into the outer layer of the colon, the prognosis is excellent. Colon cancer that spreads beyond the colon is associated with a lower risk of long term cancer-free survival.
Additional Info
American Cancer Society (ACS)
1599 Clifton Road, NE
Atlanta, GA 30329-4251
Toll-Free: (800) 227-2345
http://www.cancer.org/
National Cancer Institute (NCI)
U.S. National Institutes of Health
Public Inquiries Office
Building 31, Room 10A03
31 Center Drive, MSC 8322
Bethesda, MD 20892-2580
Phone: (301) 435-3848
Toll-Free: (800) 422-6237
TTY: (800) 332-8615
http://www.nci.nih.gov/
