No products in the cart.

Patient Basics: Hiatal Hernia
Originally published by Harvard Health.
What Is It?
A hernia occurs when part of an internal organ or body part protrudes through an opening into an area where it shouldn’t. A hiatal hernia is named for the hiatus, an opening in the diaphragm between your chest and your stomach. Normally, the esophagus (the tube that carries food to the stomach) goes through this opening. In a hiatal hernia, part of the stomach and/or the section where the stomach joins the esophagus (called the gastroesophageal junction) slips through the hiatus into the chest.
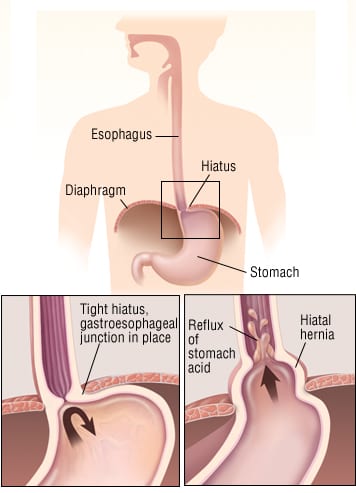
There are two types of hiatal hernias:
- Sliding — A part of the stomach and the gastroesophageal junction slip into the chest. Sliding hiatal hernias are common, especially in smokers, overweight people and women older than 50. These hernias are related to naturally occurring weaknesses in the tissues that normally anchor the gastroesophageal junction to the diaphragm and to activities or conditions that increase pressure within the abdomen. These activities or conditions include persistent or heavy coughing, vomiting, straining while defecating, sudden physical exertion and pregnancy.
- Paraesophageal — The gastroesophageal junction remains in its proper place, and a fold of the stomach slips into the chest, pinched between the gastroesophageal junction and the diaphragm. Of the two types of hiatal hernias, paraesophageal hernias are more likely to cause severe symptoms.
Symptoms
Sliding hiatal hernias may not cause any symptoms, or they may cause heartburn that is worse when you lean forward, strain or lie down. There may be chronic belching and, sometimes, regurgitation (backflow of stomach contents into the throat).
In some cases, a paraesophageal hernia may slide into the chest and become trapped (incarcerated) and unable to slide back into the abdomen. If this happens, there is a danger that the trapped hernia may die because its blood supply is cut off (strangulated). Symptoms of a strangulated hiatal hernia include sudden severe chest pain and difficulty swallowing. This situation requires immediate medical treatment.
Occasionally a hiatal hernia can cause anemia from bleeding. This can occur if the wall of the stomach becomes raw from rubbing against the edges of the diaphragm hiatus.
Diagnosis
Your doctor will ask about any history of heartburn or chest discomfort, especially if it seems to be related to eating a heavy meal, bending forward or lifting heavy objects.
Your doctor may suspect that you have a hiatal hernia based on your symptoms and risk factors (age, obesity, smoking, occupation that requires heavy lifting). To confirm the diagnosis, your doctor may order one or more of the following tests:
- Chest X-ray — A simple X-ray may show a large hiatal hernia.
- Esophagoscopy — A viewing tube is inserted down the throat to inspect the esophagus.
- Barium swallow — You swallow a fluid containing barium, which appears white on an X-ray. The path of the barium can outline the position of the hernia in the chest, or it can show that stomach contents are leaking backwards into the esophagus.
- Manometry — This test measures pressure, to diagnose abnormal muscle movements inside the esophagus.
Because many people with hiatal hernias are in the same age group that commonly experiences coronary artery disease and because the symptoms of the two disorders may be very similar, your doctor may order an electrocardiogram (EKG).
Expected Duration
In some people, a hiatal hernia slowly worsens over time and eventually requires treatment. In other people, however, the condition never causes symptoms, never gets worse and never has a significant impact on health or life.
Prevention
It is difficult to prevent a hiatal hernia. However, you can reduce your risk by maintaining a healthy weight and not smoking. To prevent a hernia associated with increased abdominal pressure, avoid activities that cause abdominal strain, especially heavy lifting. If you frequently need to strain when you move your bowels, speak to your doctor. Your doctor may prescribe stool-softening medication or suggest that you modify your diet to include more high-fiber foods.
Treatment
Most people with hiatal hernias do not require treatment. When a hiatal hernia is associated with reflux symptoms, such as heartburn, you should eat smaller, more frequent meals; avoid eating for at least two hours before going to bed; and sit up for at least one hour after eating. If lifestyle changes do not relieve the symptoms, your doctor will suggest antacids or acid blockers. Many products are on the market, including both over-the-counter and prescription medications. Fewer than 5% of people require surgery. You may need surgery to repair the hernia if you have persistent reflux symptoms or inflammation of the esophagus (esophagitis) that does not heal with medication. Your doctor may advise surgery for a paraesophageal hernia that has a risk of becoming trapped (incarcerated).
When To Call a Professional
Call your doctor if you have persistent heartburn or difficulty swallowing or feel short of breath after a meal. Call your doctor immediately if you develop heartburn accompanied by nausea, vomiting, shortness of breath, palpitations, dizziness or an irregular heartbeat. These may be signs of a heart problem rather than of a hiatal hernia or other digestive disorder.
Prognosis
The outlook is excellent. Most people with hiatal hernias have few, if any, symptoms. More bothersome symptoms usually are controlled with medications.
Additional Info
National Digestive Diseases Information Clearinghouse (NDDIC)
2 Information Way
Bethesda, MD 20892-3570
Toll-Free: 1-800-891-5389
Phone: 301-654-3810
Fax: 301-907-8906
http://digestive.niddk.nih.gov/
American College of Surgeons (ACS)
633 North Saint Clair St.
Chicago, IL 60611-3211
Phone: 312-202-5000
Toll-Free: 1-800-621-4111
Fax: 312-202-5001
http://www.facs.org/