No products in the cart.

Patient Basics: Thyroidectomy
Originally published by Harvard Health.
What Is It?
Thyroidectomy is the surgical removal of part or all of the thyroid gland. This important gland, located in the lower front portion of the neck, produces thyroid hormone, which regulates the body’s production of energy. A healthy thyroid gland is shaped like a butterfly, with right and left lobes connected by a bridge called the thyroid isthmus. Depending on the reason for a thyroidectomy, all or part of the thyroid gland will be removed. The various types of thyroidectomy include:
- Partial thyroid lobectomy (a rare procedure) — Only part of one thyroid lobe is removed.
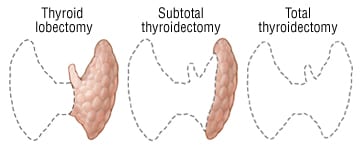
- Thyroid lobectomy — All of one thyroid lobe is removed.
- Thyroid lobectomy with isthmusectomy — All of one thyroid lobe is removed, together with the section between the two lobes (called the thyroid isthmus).
- Subtotal thyroidectomy — One thyroid lobe, the isthmus and part of the second lobe are removed.
- Total thyroidectomy — The entire thyroid gland is removed.

A thyroidectomy may be performed by using a conventional surgical approach or a newer endoscopic method done through very small incisions.
What It’s Used For
Conventional thyroidectomy is done for the following reasons:
- To remove malignant (cancerous) thyroid tumors
- To treat thyroid storm, a condition in which an overactive thyroid gland produces extremely high levels of thyroid hormone that cannot be easily controlled
- To remove all or part of a goiter (an enlarged thyroid gland) that is pressing on neighboring structures in the neck, especially if this pressure interferes with swallowing or breathing
- To remove and evaluate a thyroid nodule that on biopsy has had repeated “indeterminate” readings
In some people, as an alternative to a conventional thyroidectomy, an endoscopic thyroidectomy can be done to remove small thyroid cysts or small benign thyroid nodules (less than 4 centimeters, or about 1 ½ inches). Endoscopic thyroidectomy is not used to treat multiple thyroid nodules, thyroid cancer or thyroid storm.
Preparation
About one week before surgery, you will be told to stop taking aspirin and other blood-thinning medications. To reduce the risk of vomiting during surgery, you will be told not to eat or drink anything after midnight the night before surgery. As part of the general preparations for surgery, your doctor will review your allergies and your medical and surgical histories. If you may be pregnant, you must tell your doctor before surgery. Because you will be having a procedure that involves an area above your shoulders, you will be asked to remove all necklaces and earrings before you are taken to the operating room.
How It’s Done
Both types of thyroidectomy are usually done under general anesthesia. However, if general anesthesia is too risky for a patient, local or regional anesthesia may be used to permit the patient to remain awake during the procedure. An intravenous (IV) line will be inserted into one of your veins to deliver fluids and medications.
- Conventional thyroidectomy — In a conventional thyroidectomy, a 3- to 4-inch incision will be made through the skin in the low collar area of your neck (the lower front portion of your neck, above the collarbones and breast bone). Next, a vertical cut will be made through the strap-like muscles located just below the skin, and these muscles will be spread aside to reveal the thyroid gland and other deeper structures. Then, all or part of your thyroid gland will be cut free from surrounding tissues and removed. During the entire procedure, the surgeon will pay attention to the location of the parathyroid glands (two pairs of small glands located near the thyroid). The surgeon will focus on preserving them, if possible. After your thyroid gland is removed, one or two stitches will be used to bring your neck muscles together again. Then the deeper layer of your incision will be closed with stitches, and your skin will be closed with sterile paper tapes. A small suction catheter (tube) will be inserted near the area of your incision to drain any blood accumulated inside your neck. Following surgery, you will be taken to a recovery room, where you will be monitored for several hours until you are stable enough to return to your hospital room. After about 24 hours, the suction catheter will be removed from your neck. Most patients go home one or two days after the surgery.
- Endoscopic thyroidectomy — A viewing instrument called an endoscope and small surgical instruments will be inserted into your neck through three or four small incisions. Each incision is about 3 millimeters to 5 millimeters long (less than ¼ inch). Then the surgeon will use a tiny camera on the endoscope to guide the instruments and remove your thyroid tissue. At the end of the procedure, your neck incisions will be closed with tiny stitches or surgical tape.
Follow-Up
About one week after you return home from the hospital, you will visit your doctor for follow-up. At this visit, your doctor will check the healing of your incision or incisions. After thyroid surgery, you may need periodic blood tests to measure your thyroid hormone levels. Calcium and phosphorus levels are checked to evaluate the function of your parathyroid glands, which sometimes are damaged during thyroid surgery. If all of your thyroid gland was removed, you can expect to take thyroid supplements for the rest of your life. You may have more pain after surgery if you had a conventional thyroidectomy than if you had an endoscopic thyroidectomy. However, most patients are not good candidates for endoscopic thyroidectomy because of the type or extent of their thyroid disease.
Risks
Thyroidectomy is generally a safe surgical procedure. However, some people have major or minor complications. Possible complications include:
- Hemorrhage (bleeding) beneath the neck wound — If this occurs, the wound bulges and the neck swells, possibly compressing structures inside the neck and interfering with breathing. This is an emergency.
- Thyroid storm — If a thyroidectomy is done to treat a very overactive gland, there may be a surge of thyroid hormones into the blood. This is a very rare complication because medications are given before surgery to prevent this problem.
- Injury to the recurrent laryngeal nerve — Because this nerve supplies the vocal cords, injury can lead to vocal cord paralysis and can produce a husky voice, either short term or long term.
- Injury to a portion of the superior laryngeal nerve — If this occurs, patients who sing may not be able to hit high notes, and the voice may lose some projection.
- Wound infection
- Hypoparathyroidism — If the parathyroid glands cannot be saved or are damaged during surgery, the person may not be able to make enough parathyroid hormone. Parathyroid hormone helps keep blood calcium levels in the normal range. Low parathyroid hormone output causes low blood calcium levels.
When To Call A Professional
Once you return home from the hospital, call your doctor immediately if:
- You develop a fever.
- Your incision or any part of your neck becomes red, tender or swollen.
- Your voice seems to be hoarse, husky or weak.
- You develop symptoms of a low blood calcium level, such as numbness around your mouth, tingling in your extremities, or spasms in your feet, hands or face.
Additional Info
American Thyroid Association, Inc.
6066 Leesburg Pike
Suite 650
Falls Church, VA 22041
Phone: 703-998-8890
Fax: 703-998-8893
http://www.thyroid.org/
National Library of Medicine (NLM)
8600 Rockville Pike
Bethesda, MD 20894
Phone: 301-594-5983
Toll-Free: 1-888-346-3656
Fax: 301-402-1384
http://www.nlm.nih.gov/

