

![Novel biodegradable sirolimus-eluting stents non-inferior to durable everolimus-eluting stents [BIOSCIENCE trial]](https://www.2minutemedicine.com/wp-content/uploads/2014/09/Taxus_stent_FDA-e1607803635904-75x75.jpg)


{kind=link}


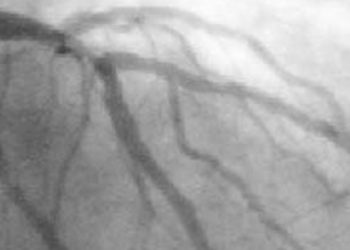
Radial artery access for invasive management of acute coronary syndrome reduces mortality and major bleeding [MATRIX Access trial]
1. In patients with acute coronary syndrome, radial artery access for coronary angiography followed by percutaneous coronary intervention significantly decreased all-cause mortality and major bleeding, compared to femoral artery access.
2. The rates of myocardial infarction and stroke were not significantly different between radial and femoral artery access
Evidence Rating Level: 1 (Excellent)
Study Rundown: As the use of invasive heart catheterization and antithrombotic therapies has increased, causing reduced risk of recurrent myocardial infarctions, the risk of bleeding has also increased, causing worse short and long-term outcomes. Heart catheterization access through the radial artery is more technically difficult than with the femoral artery due to being more superficial and smaller, but allows for better control of hemostasis, although it is unknown if radial artery access actually reduces adverse outcomes. This study randomly assigned patients with acute coronary syndrome undergoing coronary angiography and possibly percutaneous coronary intervention to receive either transradial or transfemoral artery access, comparing adverse cardiovascular events and net adverse clinical events.
The results showed that that major adverse cardiovascular events were not significantly reduced with radial artery compared to femoral artery access, while net clinical events were significantly reduced with radial artery access, mainly by a decreased risk in all-cause mortality and reduced major bleeding. Additionally, radial artery access was significantly associated with reduced rates of surgical access site repair or blood transfusion. However, there was no significant difference in rates of myocardial infarction and stroke between radial and femoral artery access. This study was strengthened by the large sample size and the use of operators experienced with a high-volume of transradial catheterizations. Limitations of this study include that secondary outcomes such as all-cause mortality did not have adjusted α levels as the primary outcomes did and thus should be interpreted cautiously.
Click to read the study in The Lancet
In-Depth [randomized controlled trial]: The Minimizing Adverse Hemorrhagic Events by TRansradial Access Site and Systemic Implementation of angioX (MATRIX Access) trial enrolled 8,404 patients with acute coronary syndrome, with or without ST-elevation myocardial infarction, who were randomly assigned to receive radial (n=4,197) or femoral (n=4,207) access during coronary angiography and possibly percutaneous coronary intervention. The primary outcomes were defined as major adverse cardiovascular events, consisting of all-cause mortality, myocardial infarction, or stroke; and net adverse clinical events, consisting of major bleeding (Bleeding Academic Research Consortium [BARC] type 3 or 5) or major adverse cardiovascular events.
Major adverse cardiovascular events occurred in 369 (8.8%) patients with radial access compared to 429 (10.3%) with femoral access (Rate ratio [RR] 0.85, 95% Confidence Interval [CI] 0.74-0.99; p=0.03037), which was non-significant due to a predefined α of 0.025. However, net clinical adverse events were significantly different, occurring in 410 (9.8%) patients with radial access compared to 486 (11.7%) patients with femoral access (RR 0.83, 95% CI 0.73-0.96; p=.0092). Radial access was associated with a significantly decreased risk of all-cause mortality (p=0.045) and major bleeding (p=0.0128), but the rates of myocardial infarction (p=0.20) and stroke (p=1.00) were not significantly different between radial and femoral access.
Image: CC/Wiki
©2015 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports
