


![Radiofrequency catheter ablation effective as first-line therapy for atrial fibrillation [RAAFT-2 trial]](https://www.2minutemedicine.com/wp-content/uploads/2014/02/afib_-75x75.jpg)
{kind=link}


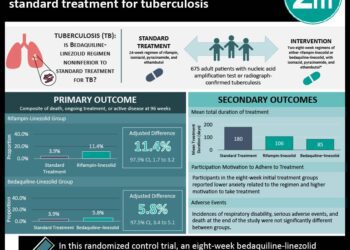
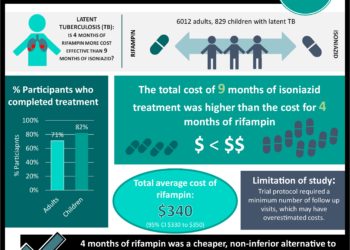
Short course rifamycin matches isoniazid for treatment of tuberculosis
1. A network meta-analysis comparing different treatment regimens for latent tuberculosis infections (LTBI) found that treating with rifamycin for 3 or more months may be an effective alternative to monotherapy and extended therapy with isoniazid (INH).
Evidence Rating Level: 1 (Excellent)
Study Rundown: Treatment regimens for latent tuberculosis infections (LTBI) have been shown efficacious and safe. However, these treatments are lengthy. The most common treatment approach consists of 6 to 9 months of INH monotherapy. Recently, a weekly combination of INH-rifapentine (RPT) for 12 weeks under direct observation was recommended. Additionally, short courses of rifampin (RMP) monotherapy for 3-4 months have been reported to be at least as effective as INH and with higher compliance rates. This study used a network meta-analysis to summarize clinical trials evaluating different LTBI treatment regimens and to provide a comparison of relative efficacies and adverse event (AE) profiles. For this mixed-treatment comparison the authors focused on randomized, controlled trials (RCTs) with end points of hepatotoxicity or development of active TB. Analysis showed improved efficacy and low hepatotoxicity profile for therapies containing rifamycin over INH, with 3-4 months of RMP monotherapy ranking highly in both domains. Overall, the results of this study suggest that regimens containing rifamycin may be just as, if not more, effective than INH monotherapy, and that these therapies should be considered in light of the need for shorter, effective, and well-tolerated treatments. Limitations to this analysis include the lack of data for some of the comparisons. Risk of bias was also unclear for many studies. Finally, the indirect comparisons allow inferences for ranking efficacy and safety, but they do not offer quantifiable clinical value.
Click to read the study, published today in the Annals of Internal Medicine
Relevant Reading: Latent Tuberculosis Infection: A Guide for Primary Health Care Providers
In-Depth [meta-analysis]: This study systematically reviewed literature through the end of January 2014 to find randomized, controlled trials that evaluated human LTBI treatment and recorded at least one of either hepatotoxicity or prevention of active TB. Of 1,516 articles identified, 53 studies met inclusion criteria and provided information on 15 regimens for comparison. 25 studies had extractable data on hepatotoxicity while 45 had data on progression to active TB. As a result, of the 105 possible regimen comparisons, only 42 (40%) had sufficient data. Odds ratios with 95% credibility intervals were calculated for all regimens vs placebo from the mixed-treatment comparison network. Regimens of INH for 6 months (OR, 0.64 [CrI, 0.48 to 0.83]) or 12-72 months (OR, 0.52 [CrI 0.41 to 0.66]), RMP for 3-4 months (OR, 0.41 [CrI 0.18 to 0.86]}, RPT-INH (OR, 0.61 [CrI, 0.29 to 1.22]), and RMP-INH (OR, 0.52 [CrI, 0.34 to 0.79]) were efficacious versus placebo. Stratifying results by immunosuppression, HIV status, and TB incidence did not affect conclusions. Neither did subgroup analysis by year, adherence, and age.
Because of limited data available for hepatotoxicity, direct comparisons were presented in the paper (data from the network meta-analysis was largely consistent). RMP only and RPT-INH regimens had lower hepatotoxicity than INH regimens of any duration. RMP-INH had lower toxicity versus INH of 12-72 months.
More from this author Expanded screening and new treatments may reduce hepatitis C burden
Image: PD
©2012-2014 2minutemedicine.com. All rights reserved. No works may be reproduced without expressed written consent from 2minutemedicine.com. Disclaimer: We present factual information directly from peer reviewed medical journals. No post should be construed as medical advice and is not intended as such by the authors, editors, staff or by 2minutemedicine.com. PLEASE SEE A HEALTHCARE PROVIDER IN YOUR AREA IF YOU SEEK MEDICAL ADVICE OF ANY SORT.
RelatedReports
