
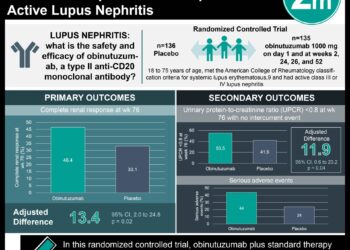
[Physician Comment] Statins associated with reduced mortality in pneumonia-related hospitalizations
Image: PD. S.pneumo
Study author, Dr. Eric Mortensen, talks to 2 Minute Medicine: Associate Professor of Internal Medicine and Clinical Sciences and Chief of General Internal Medicine at the VA North Texas Health Care System
 Why is your study is clinically important to physicians?
Why is your study is clinically important to physicians?
“First because it supports the safety of both statins and ACEI/ARBs in patients with pneumonia. As long as there are no other contraindications these medications may be continued during hospitalization for pneumonia, which may at least help prevent cardiac events. Also it suggests that these medications may, pending future research, be useful to prescribe in those who are hospitalized with pneumonia but not on them already.”
How are your findings are relevant to medical students in training?
“That many medications that we prescribe have both unintended benefits and harms. For example I originally came up with the idea for this study when I was told you must stop statins in patients with infections as some poorly designed prior studies linked low LDL to risk of death for patients with infections. This is probably as debilitated and undernourished patients have low LDLs and die more often from infection. The other way that I got the idea for this study was after listening to a cardiologist describe how statins have immunomodulatory properties, which even now are still being elucidated.”
What are the future implications of your research?
“What is needed now are randomized clinical trials to examine whether or not starting these medications at time of admission is useful for patients with pneumonia.”
Key study points:
1. Statin use prior to and during admission for pneumonia is associated with improved outcomes, including reduced 30-day mortality and length of stay.
2. ACE-I and ARBs are also associated with improved pneumonia-related outcomes, although to a lesser extent.
Primer: HMG-CoA inhibitors (statins), angiotensin converting enzyme inhibitors (ACE-I) and angiotensin receptor blockers (ARBs) are among the most common medications prescribed today. Statins are lipid-lowering drugs that are cardioprotective for patients with dyslipidemia, while ACE-I and ARBs both primarily act on the renin-angiotensin-aldosterone system to cause vasodilation and improved outcomes in patients with hypertension or congestive heart failure. Recent evidence suggests that these drugs may additionally have an effect on the immune system, modulating cytokine activity – although concrete data on mortality is conflicting. IIt is therefore currently unclear whether outpatient statin, ACE-I or ARB regimens should be started or continued inpatient when a patient is hospitalized with an infection.
This study employs a population-based retrospective study approach to assess the association between prior and inpatient use of statins, ACE-I and ARBs and clinical outcomes of patients hospitalized with pneumonia.
Background reading:
1. The effect of statins on mortality in patients with bacteremia
2. Continuation of statin therapy in patients with presumed infection: a randomized controlled trial
This [retrospective cohort] study employed the VA Health Care System database to identify patients over 65 years of age who were hospitalized from for pneumonia. Patients were stratified by use of statins, ACE-I and ARBS, and by whether each medication class was used while inpatient. Outcomes evaluated included 30-day mortality, requirement for mechanical ventilation, and length of inpatient stay.
Prior use of statins was significantly related to a decreased 30-day mortality, as was continued use of statin therapy inpatient. Statin use was also significantly associated with decreased need for mechanical ventilation and decreased length of hospital stay. ACE-I was also associated with reduced mortality as well as shorter hospitalization, however only ACE-I use inpatient showed a statistically significant association. Similarly, use of ARBs was significantly related to a reduction in mortality, but only inpatient use of ARBs showed a statistically significant reduction in hospital stay. Neither ACE-I nor ARB use was associated with the need for ventilation.
In sum: Statins, ARBs and ACE inhibitors are associated with improved outcomes in patients ≥ 65 years hospitalized with pneumonia. The data shows the strongest associations between statins and reduced mortality, decreased use of mechanical ventilation and reduction in length of stay, both prior to and during inpatient hospital stay. This study suggests that there is no risk in inpatient continuation of statins, ACE-I or ARBs previously prescribed to a patient who is hospitalized for pneumonia, and that there may be an overall benefit to their continuation.
As a retrospective study, only associations can be highlighted. Randomized trials are, as usual, needed to establish causality. Additionally, the study subjects are predominantly men and the study was limited to patients over 65 years of age, so these conclusions may not be generalizable to other patient populations.
The medications studied have many effects on the body, including, but not limited to, cardiovascular effects, cytokine modulation, effects on coagulation, and on nitric oxide balance. It is not clear from this data which, if any, of these processes is directly responsible for the improved outcomes. Further investigation to elucidate the mechanism by which these drugs show increased benefit in patients with pneumonia and other infectious processes is needed.
Click to read the study in Clinical Infectious Diseases
By [EH] and [MS]
© 2012 2minutemedicine.com. All rights reserved. No works may be reproduced without written consent from 2minutemedicine.com. Disclaimer: We present factual information directly from peer reviewed medical journals. No post should be construed as medical advice and is not intended as such by the authors or by 2minutemedicine.com. PLEASE SEE A HEALTHCARE PROVIDER IN YOUR AREA IF YOU SEEK MEDICAL ADVICE OF ANY SORT.


![[Physician Comment] The extent of C. difficile infections may not differ in light of immune status](https://www.2minutemedicine.com/wp-content/uploads/2012/11/x800px-Clostridium_difficile_01-e1353335581537.jpg.pagespeed.ic_.We5DxZl6Ye-75x75.jpg)