



{kind=link}


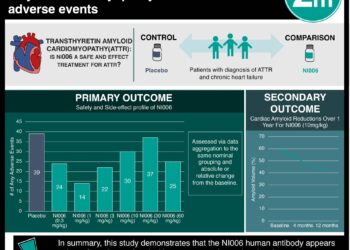
Tafamidis attenuates the decline of cardiac function in patients with transthyretin amyloid cardiomyopathy
1. Patients with transthyretin amyloid cardiomyopathy (ATTR-CM) managed with tafamidis showed decreased worsening in left ventricular (LV) systolic and diastolic function over 30 months compared to the placebo group.
2. Approximately half of the subjects enrolled in the Tafamidis in Transthyretin Cardiomyopathy Clinical Trial (ATTR-ACT) exhibited various levels of diminished left ventricular ejection fraction (LVEF), underscoring the importance of considering ATTR-CM as a potential diagnosis in individuals with heart failure, irrespective of the underlying LVEF.
Evidence Rating Level: 1 (Excellent)
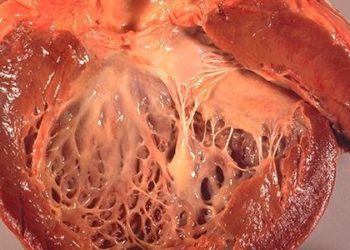
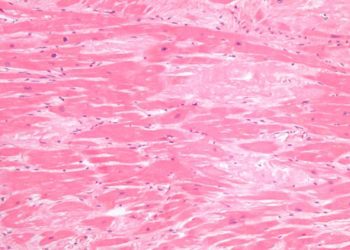
Study Rundown: ATTR-CM is a fatal condition resulting from the accumulation of transthyretin amyloid fibrils in the myocardium, leading to cardiomyopathy and heart failure symptoms. Untreated ATTR-CM has a poor prognosis, the disease manifests with increased ventricular wall thickness and diastolic dysfunction due to amyloid deposits. In the ATTR-ACT, tafamidis demonstrated significant benefits, reducing mortality, cardiovascular-related hospitalizations, and the decline in functional capacity and quality of life compared to placebo. Despite recognized clinical benefits, the impact of tafamidis on echocardiographic parameters measuring cardiac function remains incompletely characterized, with recent single-center studies suggesting a potential attenuation of cardiac function decline in patients treated with tafamidis compared to patients who have never taken the drug. The goal of this post hoc analysis of the ATTR-ACT was to elucidate the underlying factors contributing to improved survival with tafamidis, administered at the approved dose for ATTR-CM (80 mg). This was done by evaluating the echocardiographic measures recognized as prognostic factors for mortality in ATTR-CM of both the drug group and placebo group. They found that over 30 months, patients with ATTR-CM treated with tafamidis exhibited a reduction in the deterioration of LV and diastolic function compared to the placebo group. One strength of this study was its utilization of a core laboratory to ensure a standardized evaluation of echocardiographic data, enhancing the reliability and consistency of the assessments across the study participants and contributing to the overall robustness of the research. In conclusion, these clinical observations underscore the importance of early diagnosis and intervention in individuals with ATTR-CM to mitigate the progressive deterioration of cardiac function.
Click to read the study in JAMA Cardiology
Relevant Reading: Tafamidis Treatment for Patients with Transthyretin Amyloid Cardiomyopathy
In-Depth [randomized controlled trial]: This study is a post hoc analysis of the ATTR-ACT, an international, multicenter, double-blind, placebo-controlled phase 3 randomized clinical trial of tafamidis for ATTR-CM conducted between December 2013 to February 2018. Patients aged 18 to 90 with biopsy-confirmed ATTRv-CM (hereditary) or ATTRwt-CM (wild type), a history of heart failure, and end-diastolic interventricular septal wall thickness of 12mm or greater were randomized 2:1:2 to receive once-daily oral tafamidis meglumine (80mg), tafamidis meglumine (20mg), or matching placebo for 30 months. The primary analysis involved comparing alterations in LVEF, LV stroke volume (LVSV), LV global longitudinal strain (LVGLS), and septal and lateral E/e’ at baseline, 6 months, 18 months, and 30 months among the tafamidis (80mg) and placebo groups. Additionally, changes in regional measures of LV longitudinal, circumferential, and radial strain, as well as left atrial diameter from baseline to month 30, were examined between the treatment groups. The longitudinal analyses specifically focused on patients receiving tafamidis (80mg), as it represents the approved dose for ATTR-CM. Among 436 patients with available echocardiographic data, 50.5% had heart failure with preserved LV ejection fraction, 27.3% had mildly reduced, and 22.2% had reduced ejection fraction. Over 30 months, individuals receiving tafamidis (80mg) experienced less significant deterioration in four echocardiographic measures compared to those on placebo (176 patients vs. 177 patients): LVSV (least squares mean difference: 7.02 mL; 95% CI, 2.55-11.49; P = 0.002), LVGLS (−1.02%; 95% CI, −1.73 to −0.31; P = 0.005), septal E/e′ (−3.11; 95% CI, −5.50 to −0.72; P = 0.01), and lateral E/e′ (−2.35; 95% CI, −4.01 to −0.69; P = 0.006). A decrease in LVEF became evident starting from month 6 with the placebo group, while there was minimal decline observed with tafamidis (80mg) until month 30. There were no significant interactions between the impact of tafamidis (80mg) and baseline LVEF across various outcomes, including all-cause mortality (P = 0.40), cardiovascular-related hospitalizations (P = 0.35), and changes in specific echocardiographic parameters.
Image: PD
©2023 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports
