
The BHAT: Propranolol after acute myocardial infarction [Classics Series]
1. Beta-blockers were commonly used in the treatment of coronary artery disease in the 1980s, though prior studies were inconclusive due to limitations in study design and small sample sizes.
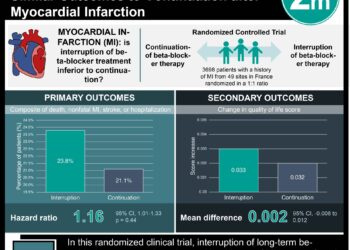
2. This was the first large, randomized trial to demonstrate that propranolol significantly reduced mortality after acute myocardial infarction when compared with placebo.
Original Date of Publication: March 1982
Study Rundown: The Beta-Blocker Heart Attack Trial (BHAT) was established in 1977 to study whether daily administration of propranolol after a myocardial infarction would lead to a reduction in total mortality. Prior to this study, beta-blockers were well known to reduce myocardial oxygen demand and suppress arrhythmias. They were also widely used in the setting of coronary artery disease, although numerous studies exploring this question were inconclusive due to small sample sizes and study design issues.
In summary, patients with recent hospitalization for myocardial infarction experienced significantly lower all-cause mortality when taking propranolol rather than placebo. Moreover, propranolol therapy led to significantly lower rates of cardiovascular mortality and sudden death. Patients taking propranolol experienced significantly higher rates of bronchospasm and diarrhea, but fewer instances of palpitations when compared to placebo. The BHAT was the first large, randomized trial to demonstrate a significant reduction in mortality when treating patients with recent myocardial infarction with a beta-blocker, and beta-blockade remains a staple in the management of acute myocardial infarction.
Click to read the study in JAMA
In-Depth [randomized controlled trial]: The BHAT was a double-blinded, placebo-controlled, randomized trial conducted at 31 institutions in the United States and Canada. Patients were eligible for the study if they were between 30-69 years of age and hospitalized for acute myocardial infarction. Exclusion criteria were having a contraindication to propranolol (marked bradycardia), a history of severe heart failure or asthma, other life-threatening illness, a need for cardiac surgery, or a previous need for beta-blocker therapy. A total of 3837 were enrolled and randomized to treatment with propranolol 40 mg every eight hours or placebo. The propranolol dose was subsequently titrated up to 60 mg or 80 mg every eight hours.
The majority of patients enrolled in this study were white males, comprising over 80% of the study population. Compared with patients who received placebo, those in the propranolol group experienced significantly lower all-cause mortality (7.2% vs. 9.8%, p < 0.005). Patients taking propranolol also experienced significantly lower cardiovascular mortality (6.6% vs. 8.9%, p < 0.01), arteriosclerotic heart disease mortality (6.2% vs. 8.5%, p < 0.01), and sudden death (3.3% vs. 4.6%, p < 0.05) compared to those treated with placebo.
There were significantly more instances of bronchospasm (31.3% vs. 27.0%, p < 0.005) and diarrhea (5.5% vs. 3.6%, p < 0.01) in the propranolol group, though palpitations were more common in the placebo group (10.8% vs. 15.1%, p < 0.001).
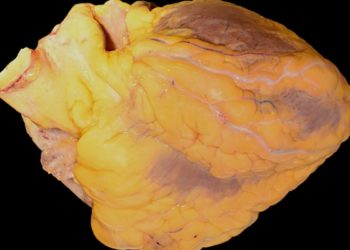
Image: PD
©2016 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.




{kind=link}