No products in the cart.

Child-Pugh Score: Prognosis, Classification & Cirrhosis Staging in Chronic Liver Disease [Classics Series]
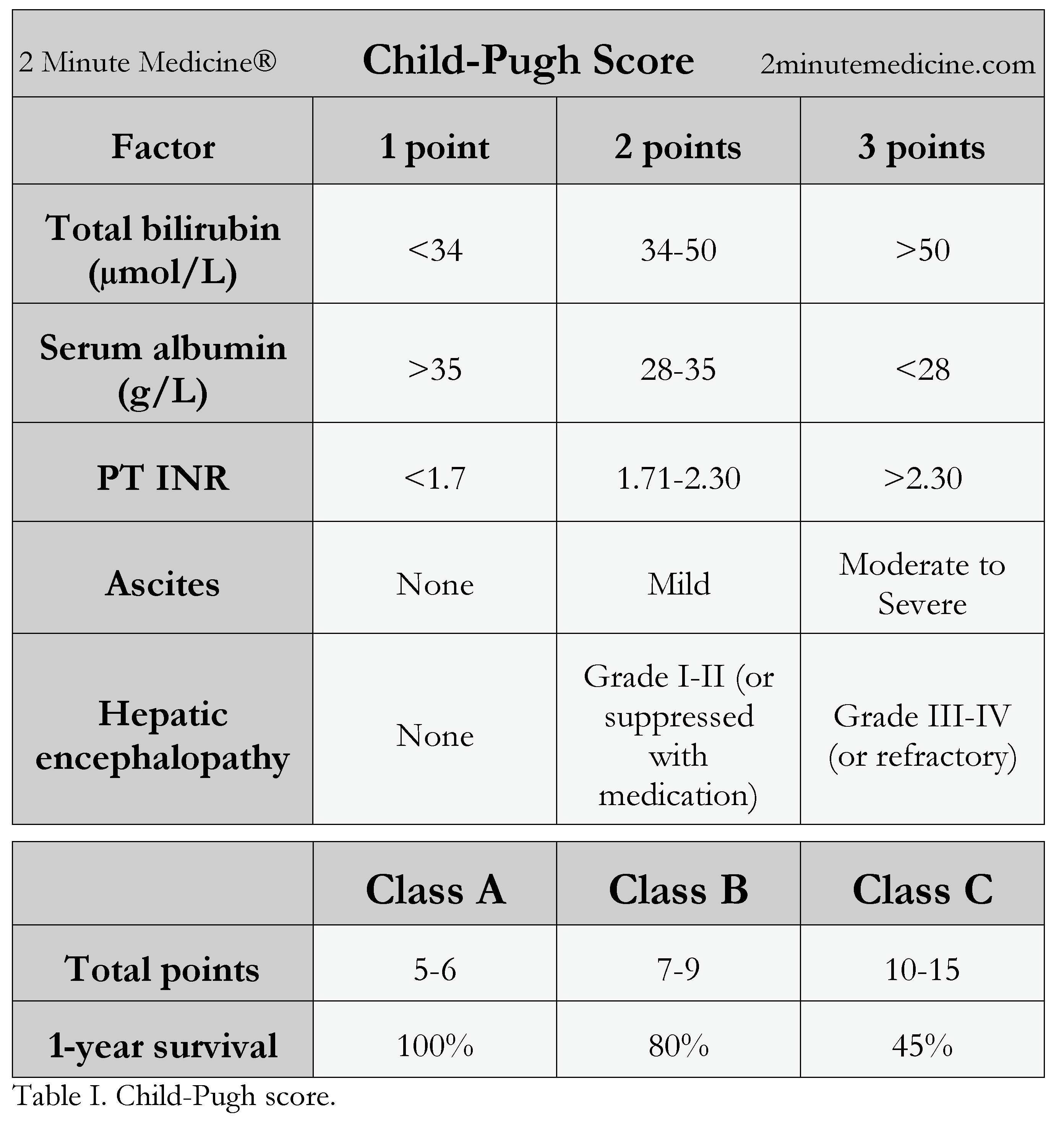
1. The Child-Pugh score, derived from five clinical and lab measures (bilirubin, albumin, INR/prothrombin time, ascites, encephalopathy), is widely used to predict operative mortality and long-term prognosis in chronic liver disease and cirrhosis.
2. First developed in 1973 to assess surgical risk in patients with bleeding esophageal varices, the Child-Pugh classification remains a cornerstone of liver disease staging and is often used alongside the MELD score to guide liver transplant prioritization.
Original Date of Publication: August 1973
This study summary is an excerpt from the book 2 Minute Medicine’s The Classics in Medicine: Summaries of the Landmark Trials, 2e (The Classics Series).
Study Rundown: The Child-Pugh score, first described by Child and Turcotte and later modified by Pugh in 1973, was designed to estimate operative mortality in patients with bleeding esophageal varices. It is calculated using five parameters: total bilirubin, serum albumin, prothrombin time or INR, the presence and severity of ascites, and the degree of hepatic encephalopathy. Each factor is assigned a score from one to three, with the total determining the class of liver disease severity. Class A, with scores of five to six, represents the best prognosis, Class B with scores of seven to nine indicates moderate impairment, and Class C with scores of ten to fifteen reflects severe functional compromise.
In the original variceal surgery cohort, operative mortality was 29 percent for Class A, 38 percent for Class B, and 88 percent for Class C. Despite its age, the Child-Pugh score is still widely applied for prognosis in cirrhosis and to help guide clinical decisions, particularly regarding surgery and transplant candidacy.
Please click to read study in British Journal of Surgery
In-Depth [case series study]: This study, originally published in 1973 in the British Journal of Surgery, sought to determine whether clinical features could help predict surgical outcomes in patients with esophageal varices. A total of 38 consecutive cases of bleeding esophageal varices requiring surgery were included in the study. The severity of liver disease was assessed in each patient based on five clinical features: 1) total bilirubin level, 2) serum albumin, 3) prothrombin time (now measured as the INR), 4) the degree of ascites, and 5) the grade of hepatic encephalopathy. The total point score was then used to determine the patient’s Child-Pugh class. Class A patients (n=7) experienced a 29% operative mortality rate, while Class B (n=13) and Class C (n=18) patients had operative mortality rates of 38% and 88%, respectively. Since its publication, the Child-Pugh score has undergone modifications and is currently used to assess the severity and prognosis of chronic liver disease and cirrhosis. Moreover, it is often used together with the MELD to determine the priority for liver transplantation. The currently used Child-Pugh scoring system has been outlined below.
Pugh RNH, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg. 1973 Aug 1;60(8):646–9.
© 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.

{kind=link}
