
The FREEDOM trial: Coronary bypass graft vs. PCI in diabetic patients [Classics Series]
1. In patients with diabetes and multivessel disease, coronary artery bypass grafting (CABG) was shown to be superior to percutaneous coronary intervention (PCI) with drug-eluting stents in reducing the risk of all-cause mortality and nonfatal myocardial infarction.
2. Patients treated with PCI experienced a smaller risk of nonfatal stroke, but also had significantly higher rates of revascularization within a year of their procedure compared to those treated with CABG.
Original Date of Publication: December 2012
Study Rundown: Patients with multivessel coronary artery disease regularly undergo revascularization, and a large portion of these patients have diabetes. Prior studies have demonstrated that diabetic patients have greater survival when they receive CABG rather than balloon angioplasty, and as a result, guidelines at the time favored CABG for revascularization. There have been significant advances in PCI over the past few decades, particularly with the advent of drug-eluting stents. As a result, it remains unclear whether CABG or PCI was more suitable for multivessel disease in the context of diabetes.
The Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease (FREEDOM) trial sought to address this question. Patients with diabetes and multivessel disease were randomized to undergo PCI with drug-eluting stents or CABG in addition to standard medical therapy, and subsequently followed for minimum of 2 years. In summary, CABG was found to be superior to PCI in reducing all-cause mortality and nonfatal myocardial infarctions in this patient population. Compared to PCI, CABG was linked with a small but significant increase in the risk of nonfatal stroke. Nevertheless, this trial supports the use of CABG over PCI in diabetic patients with multivessel disease.
Click to read the study in NEJM
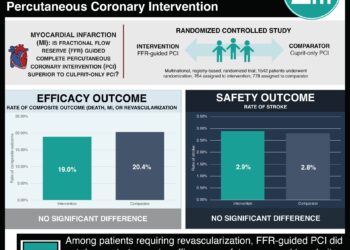
In-Depth [randomized controlled trial]: This randomized controlled trial was conducted at 140 centers around the world. To be included, patients had to have diabetes and angiographically confirmed multivessel disease with stenosis >70% in two or more major coronary arteries in at least two major coronary-artery territories. Patients with left main coronary stenosis were excluded. A total of 1900 patients met these criteria and underwent randomization to either PCI with drug-eluting stents or CABG, where arterial revascularization was encouraged. All patients were treated to optimize their medical risk factors (e.g., low-density lipoprotein levels, blood pressure, glycated hemoglobin), and the primary outcome was a composite of all-cause mortality, nonfatal myocardial infarction, and nonfatal stroke.
The rate of the primary outcome was significantly higher in patients receiving PCI than in those receiving CABG at 5 years (26.6% vs. 18.7%, absolute difference 7.9%, 95%CI 3.3 to 12.5%, p = 0.005). This was driven by lower rates of all-cause mortality (absolute difference 5.4%, 95%CI 1.5 to 9.2%, p = 0.049) and nonfatal myocardial infarction (p < 0.001). Patients treated with PCI experienced significantly fewer strokes than those treated with CABG (p = 0.03). Significantly higher rates of repeat revascularization within 1 year were observed in the PCI compared to CABG group (12.6% vs. 4.8%, p < 0.001).
Image: PD
©2016 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.



![Adverse pregnancy outcomes associated with thrombophilias [Classics Series]](https://www.2minutemedicine.com/wp-content/uploads/2015/07/Classics-2-Minute-Medicine-e1436017941513-75x75.png)

{kind=link}