
#VisualAbstract: Serum Urate Lowering with Allopurinol and Kidney Function in Type 1 Diabetes
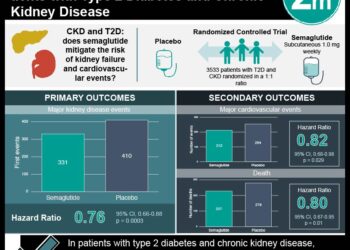
1. Urate reduction with allopurinol did not slow the decline of estimated glomerular filtration rate (eGFR) compared to the placebo treatment in patients with chronic kidney disease.
2. The urinary albumin:creatinine ratio was shown not to be significantly different between the treatment groups.
Evidence Rating Level: 1 (Excellent)
Study Rundown: Increased risk in the onset and progression of chronic kidney disease is associated with elevated serum urate levels. As a result of decreased excretion, the serum urate level increases linearly as the GFR decreases. However, it is unclear whether elevated serum urate levels exacerbate kidney disease progression or if it acts as an indirect marker for decreased kidney function. As such, this study tested whether the serum urate reduction with allopurinol would reduce the decline in the eGFR in patients with chronic kidney disease. The study determined patients with urate lowering therapy with allopurinol did not have a slower decline in eGFR compared to the patients in the placebo treatment group. This study had several limitations. Of note, the trial used a serum creatinine-based equation to calculate eGFR, which was not as sensitive in detecting GFR changes. Also, during the trial, a high percentage of patients discontinued the treatment regimen, which led to an underpowered study. Nonetheless, this study was strengthened by the prolonged follow-up period for both treatment groups.
Click to read the study, published today in NEJM
In-Depth [randomized controlled trial]: This randomized control trial enrolled 369 patients in a multicenter study from 31 sites in Australia and New Zealand. Patients who were included were at least 18 years of age, had evidence of stage 3 or 4 kidney disease and an albumin/creatinine ratio of 265 or greater. The exclusion criteria for the study included history of gout and allopurinol insensitivity. The patients were randomized in a 1:1 ratio to receive either oral placebo or allopurinol. The primary outcome was the change in eGFR from baseline to the end of the trial at 104 weeks. The change in eGFR did not significantly differ between the allopurinol group (-3.33 mL per minute per 1.73m2 per year; 95% confidence interval [CI], -4.11 to -2.55) and placebo group (-3.23 mL per minute per 1.73m2 per year; 95% CI, -3.98 to -2.47). The mean difference for the eGFR changes amongst both groups was -0.10 mL per minute per 1.73m2 per year (95% CI, -1.18 to 0.97; P=0.85). At week 104, the mean serum urate level, in the allopurinol group, decreased to 5.3 mg per deciliter (95% CI, 5.1 to 5.6), while the mean serum urate level, in the placebo group, decreased to 8.2 mg per deciliter (95% CI, 7.9 to 8.4). Furthermore, there was no significant difference in the urinary albumin:creatinine ratio between the two group (between-group difference, -9%; 95% CI, -24 to 10). Taken together, the reduction of serum urate with allopurinol did not slow the decline of eGFR in patients with chronic kidney disease.
©2020 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.


![Nanoparticle delivery of aurora kinase inhibitor may improve tumor treatment [PreClinical]](https://www.2minutemedicine.com/wp-content/uploads/2016/02/20541_lores-75x75.jpg)

{kind=link}